ABSTRACT
Hepatic angiomyolipoma (HAML) is a rare mesenchymal tumor of the liver composed of varying proportions of adipose tissue, smooth muscle cells, and blood vessels. Its heterogenous composition results in diverse features that may closely mimic hepatocellular carcinoma (HCC) on imaging. Here, we report a 56-year-old woman was referred after an incidental 1.8 cm hepatic mass on computed tomography. Magnetic resonance imaging demonstrated arterial phase hyperenhancement, portal venous washout, hepatobiliary phase hypointensity, and diffusion restriction, strongly mimicking the imaging appearance of HCC. However, the absence of chronic liver disease or viral hepatitis limited a confident noninvasive diagnosis. To establish a definitive diagnosis, percutaneous tumor biopsy was performed. Histologically, the lesion consisted showed a characteristic admixture of smooth muscle cells, adipose tissue, and blood vessels, and immunohistochemistry demonstrated diffuse positivity for HMB-45, confirming the diagnosis of HAML.
-
KEYWORDS: Angiomyolipoma; Liver; Hepatocellular carcinoma; Immunohistochemistry
INTRODUCTION
Hepatic angiomyolipoma (HAML) is a rare mesenchymal tumor belonging to the family of perivascular epithelioid cell tumors (PEComas) [
1]. Although most cases follow a benign clinical course, HAML exhibits highly variable radiologic appearances depending on the proportion of adipose tissue, smooth muscle, and vascular components [
2]. In particular, fat-poor or epithelioid-predominant HAML may demonstrate imaging features that overlap with hepatocellular carcinoma (HCC), including arterial phase hyperenhancement and delayed washout, leading to frequent misdiagnosis [
3-
5]. Accurate preoperative diagnosis of HAML remains challenging, especially in patients without chronic liver disease or established risk factors for HCC. In such settings, histopathologic confirmation with immunohistochemical staining, including HMB-45 and melanocytic markers, is essential for definitive diagnosis and appropriate management [
1,
6]. Here, we report a case of HAML that radiologically mimicked HCC in the absence of chronic liver disease or viral hepatitis and was confirmed by percutaneous biopsy, highlighting the importance of considering HAML in the differential diagnosis of hypervascular hepatic lesions.
CASE
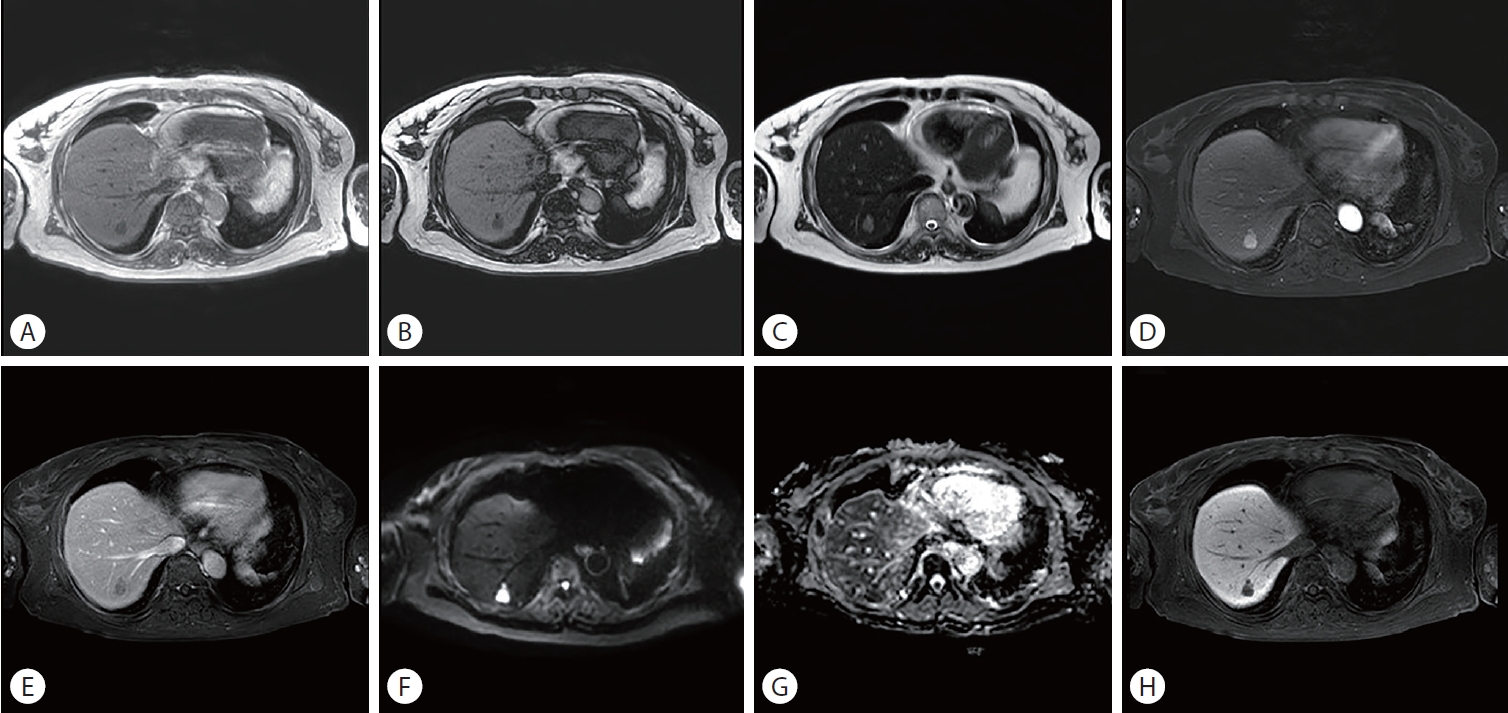
A 56-year-old woman was referred to our hepatology clinic after an incidental hepatic mass was identified on computed tomography. She had no history of chronic liver disease, viral hepatitis, or significant alcohol intake. Physical examination was unremarkable. Laboratory tests, including liver function tests, were within normal limits. Serum tumor markers, including alpha-fetoprotein, were not elevated. Contrast-enhanced magnetic resonance imaging revealed a 1.8 cm well-defined lesion located in the subcapsular area of the liver (
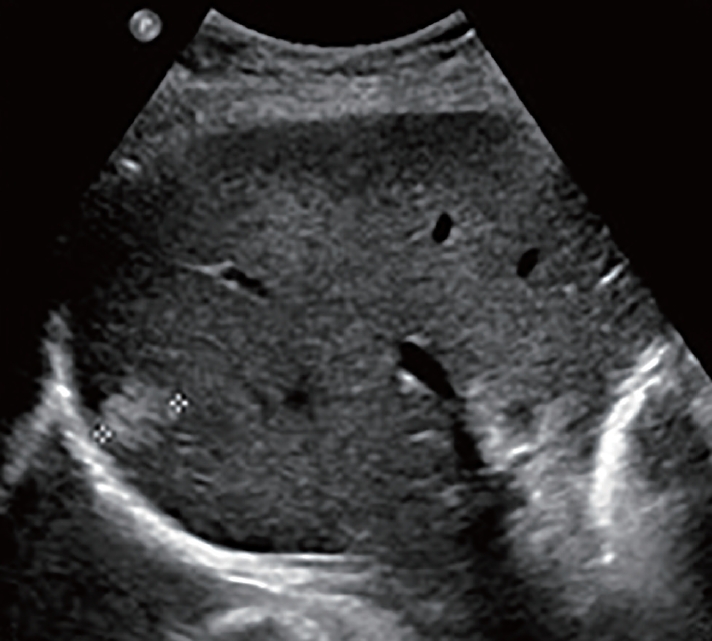
Fig. 1). The lesion demonstrated focal signal drop on opposed-phase imaging, suggesting intralesional fat. It also showed arterial phase hyperenhancement, washout on the portal venous phase, diffusion restriction, and hypointensity on the hepatobiliary phase, closely mimicking HCC on imaging. However, because the patient had no cirrhosis, chronic viral hepatitis, or prior HCC history. Given the discordance between the imaging findings and clinical background, percutaneous tumor biopsy was performed to establish a definitive diagnosis. Gray-scale transabdominal ultrasonography shows a well-defined, predominantly hyperechoic nodule in hepatic segment 7 (
Fig. 2). Histologic examination revealed a tumor composed of smooth muscle cells, adipose tissue, and blood vessels. Immunohistochemical staining showed diffuse positivity for HMB-45 in the tumor cells, confirming the diagnosis of HAML (
Fig. 3). The patient was managed conservatively with clinical and radiologic follow-up.
DISCUSSION
Angiomyolipoma is an uncommon mesenchymal tumor classified within the PEComa family [
1]. Although angiomyolipoma is most frequently encountered in the kidney, hepatic involvement is rare and represents a diagnostic challenge because its radiologic appearance is highly variable [
2]. The imaging characteristics largely depend on the relative proportion of adipose tissue, smooth muscle, and vascular components [
2]. As a result, HAML can resemble various benign and malignant hepatic tumors, and it is particularly prone to being misdiagnosed as HCC [
3].
In the present case, the lesion demonstrated arterial phase hyperenhancement with portal venous washout and diffusion restriction, which are considered typical imaging hallmarks of HCC. However, this diagnostic impression was discordant with the clinical context, as the patient had no chronic liver disease or established risk factors for HCC. Importantly, fat-poor HAML is known to mimic HCC because it may not show macroscopic fat and can exhibit hypervascularity with washout due to its prominent vascular component [
3-
5]. Although certain imaging findings may suggest HAML—such as intratumoral fat, early draining veins, aneurysmal dilatation of tumor vessels, or a capsule-like appearance—these features are inconsistent and often absent, particularly in small lesions [
2,
7]. Therefore, when a hypervascular hepatic tumor is detected in a non-cirrhotic liver and the diagnosis of HCC is uncertain, histopathologic confirmation should be considered [
3]. In our case, percutaneous biopsy enabled definitive diagnosis and prevented unnecessary surgical intervention.
Histologically, HAML is characterized by varying admixtures of epithelioid or spindle smooth muscle cells, mature adipose tissue, and abnormal thick-walled blood vessels [
1]. Immunohistochemistry is essential for diagnosis, and tumor cells typically express melanocytic markers such as HMB-45 and Melan-A, as well as smooth muscle markers including smooth muscle actin [
1,
6]. In the current case, the tumor showed the classic histologic triad and diffuse HMB-45 positivity, confirming the diagnosis.
Most HAMLs behave in a benign manner, and conservative management with imaging surveillance is generally appropriate in asymptomatic patients with small tumors [
2]. However, malignant transformation and recurrence have been reported, particularly in tumors with epithelioid predominance, large size, high mitotic activity, necrosis, or vascular invasion [
8,
9]. In the present case, histologic examination demonstrated a classic triphasic angiomyolipoma composed of smooth muscle cells, adipose tissue, and blood vessels, without evidence of high-risk features. Therefore, immediate surgical resection was not considered mandatory, and close radiologic surveillance was selected. Surgical resection may be considered in selected cases when malignancy cannot be excluded, when the lesion is symptomatic, or when high-risk pathologic features are present.
In conclusion, HAML should be included in the differential diagnosis of hypervascular hepatic lesions, especially in patients without cirrhosis or viral hepatitis. Because imaging findings may closely mimic HCC, percutaneous biopsy with appropriate immunohistochemical evaluation plays a critical role in establishing the correct diagnosis and avoiding overtreatment.
NOTES
-
ACKNOWLEDGEMENTS
None.
-
FUND
None.
-
ETHICS STATEMENT
Ethical approval was obtained from the Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 55-2026-069). The consent for publication was not required as the submission does not include any images or information that may identify the person.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Y.M.H. designed the study; Y.M.H. was responsible for the data acquisition; Y.M.H. analyzed the data; Y.M.H. wrote the first draft; Y.M.H. critically reviewed the manuscript; Y.M.H. supervised the project; All authors read and approved the final manuscript.
Figure 1.Magnetic resonance imaging. (A) In-phase T1-weighted image shows a well-defined ovoid lesion. (B) Opposed-phase image demonstrates focal signal drop within a portion of the lesion, suggesting intralesional fat. (C) T2-weighted image (T2WI) shows moderately high signal intensity. (D) Arterial phase image demonstrates arterial phase hyperenhancement. (E) Portal venous phase image shows washout of the lesion. (F) Diffusion-weighted image (DWI) shows high signal intensity of the lesion. (G) Apparent diffusion coefficient (ADC) map demonstrates corresponding low signal intensity, consistent with restricted diffusion. (H) Hepatobiliary phase image demonstrates hypointensity relative to the surrounding liver parenchyma.
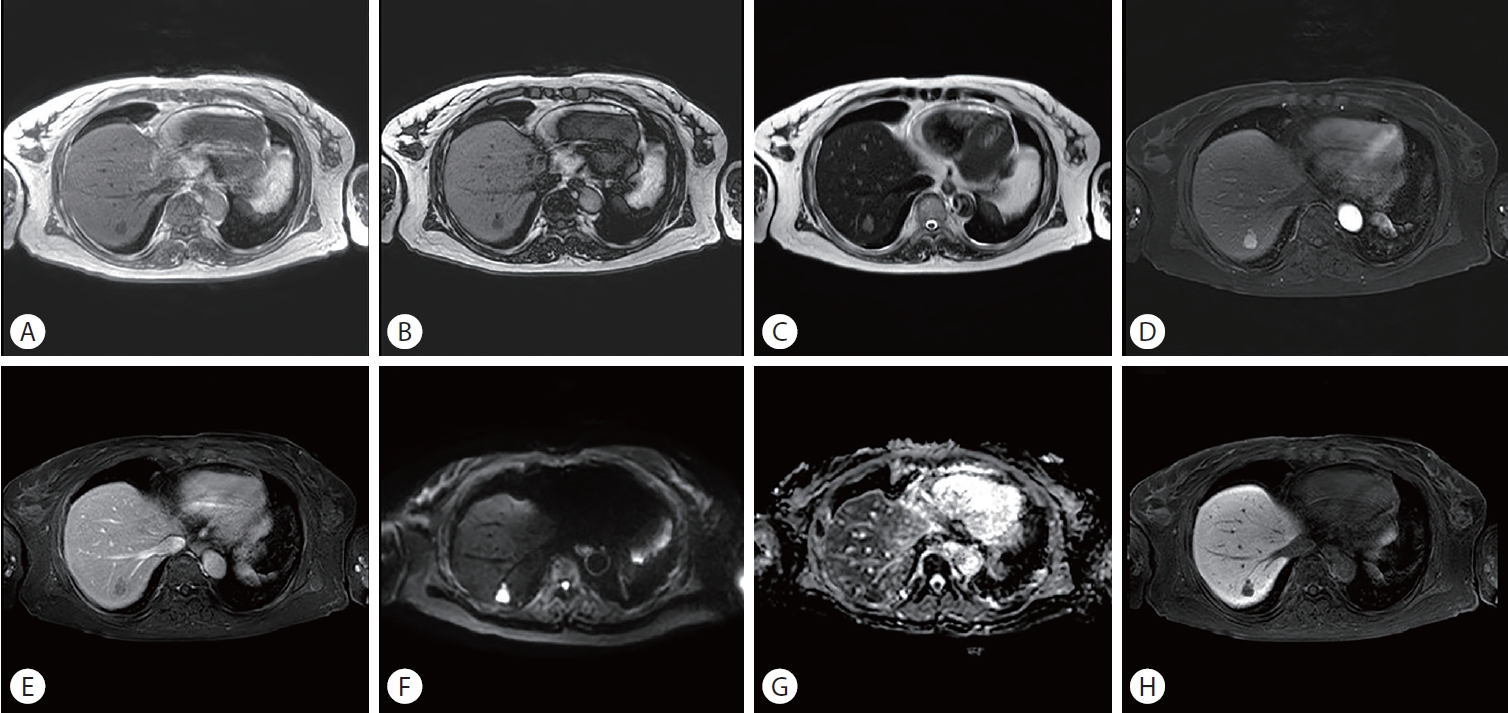
Figure 2.Sonographic finding. The lesion is a well-defined, predominantly hyperechoic nodule.

Figure 3.Histologic findings. (A) The tumor consists of smooth muscle cells, adipocytes, and entrapped hepatocytes (×200, hematoxylin and eosin [H&E] stain). (B) The other part of the biopsy specimen shows blood vessels (×200, H&E stain). (C) Smooth muscle cells express HMB45 (×200) (dashed line: border between the tumor and adjacent liver parenchyma).

REFERENCES
- 1. Folpe AL, Mentzel T, Lehr HA, Fisher C, Balzer BL, Weiss SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol 2005;29:1558-1575.
- 2. Seow J, McGill M, Wang W, Smith P, Goodwin M. Imaging hepatic angiomyolipomas: key features and avoiding errors. Clin Radiol 2020;75:88-99.
- 3. Lee SJ, Kim SY, Kim KW, et al. Hepatic angiomyolipoma with minimal fat, mimicking hepatocellular carcinoma. Clin Mol Hepatol 2012;18:330-335.
- 4. Wang CP, Li HY, Wang H, et al. Hepatic angiomyolipoma mimicking hepatocellular carcinoma: magnetic resonance imaging and clinical pathological characteristics in 9 cases. Medicine (Baltimore) 2014;93:e194.
- 5. Kim R, Lee JM, Joo I, et al. Differentiation of lipid poor angiomyolipoma from hepatocellular carcinoma on gadoxetic acid-enhanced liver MR imaging. Abdom Imaging 2015;40:531-541.
- 6. Tsui WM, Colombari R, Portmann BC, et al. Hepatic angiomyolipoma: a clinicopathologic study of 30 cases and delineation of unusual morphologic variants. Am J Surg Pathol 1999;23:34-48.
- 7. Lee SJ, Kim SY, Kim KW, et al. Hepatic angiomyolipoma versus hepatocellular carcinoma in the noncirrhotic liver on gadoxetic acid-enhanced MRI: a diagnostic challenge. AJR Am J Roentgenol 2016;207:562-570.
- 8. Garoufalia Z, Machairas N, Kostakis ID, et al. Malignant potential of epithelioid angiomyolipomas of the liver: A case report and comprehensive review of the literature. Mol Clin Oncol 2018;9:226-230.
- 9. Deng YF, Lin Q, Zhang SH, Ling YM, He JK, Chen XF. Malignant angiomyolipoma in the liver: a case report with pathological and molecular analysis. Pathol Res Pract 2008;204:911-918.
Citations
Citations to this article as recorded by