ABSTRACT
Immune checkpoint inhibitor (ICI)-based combination therapy has transformed the treatment of advanced hepatocellular carcinoma (HCC), yet immune-related adverse events (irAEs) remain a serious and potentially fatal complication. We report two cases of severe irAEs following ICIbased therapy for HCC. In Case 1, a man with multimetastatic HCC developed immune-mediated colitis with hemodynamic collapse and multi-organ failure after the second cycle of the STRIDE regimen yet achieved a near-complete oncologic response. In Case 2, a patient who had tolerated 17 cycles of adjuvant atezolizumab (ate) plus bevacizumab (bev) without irAE developed fatal immune-mediated fulminant hepatitis after a single dose of ate+bev reinitiated as first-line therapy for unresectable HCC following recurrence and TACE failure. These cases highlight the unpredictability of irAEs—even in previously tolerant patients—and underscore the importance of early recognition and prompt management.
-
KEYWORDS: Carcinoma, hepatocellular; Immune checkpoint inhibitors; Drug-related side effects and adverse reactions; Colitis; Chemical and drug induced liver injury
INTRODUCTION
Immune checkpoint inhibitor (ICI)-based combination therapy has transformed the systemic treatment landscape for unresectable hepatocellular carcinoma (HCC), with two pivotal phase III trials establishing new standards of care. In IMbrave150, atezolizumab plus bevacizumab (ate+bev) demonstrated superior overall survival compared with sorafenib (median OS 19.2 vs. 13.4 months; HR 0.66) [
1], and the HIMALAYA trial subsequently confirmed that durvalumab plus tremelimumab (STRIDE regimen) similarly improved overall survival over sorafenib (HR 0.78) [
2], offering an alternative first-line option through a distinct mechanism of dual checkpoint blockade.
Despite their efficacy, ICI-based therapies enhance immune system activity and can thereby induce a spectrum of inflammatory toxicities, collectively termed immune-related adverse events (irAEs). Although any organ system can be affected, irAEs most commonly involve the gastrointestinal tract, endocrine glands, skin, and liver, with onset typically occurring within weeks to months of treatment initiation [
3]. The type and severity of toxicities differ by regimen: in IMbrave150 [
1], immune-mediated adverse events of special interest occurred in approximately 26% of patients receiving ate+bev, with treatment-related grade 3–4 adverse events occurring in 43% of the ate+bev arm; in the HIMALAYA trial [
2], irAEs occurred in 35.8% of patients receiving STRIDE, most within the first 3 months. Although most irAEs are manageable with early intervention, grade 3–4 events can necessitate permanent ICI discontinuation and may be fatal. We herein report two cases of severe irAEs—immune-related colitis and fulminant hepatitis—following distinct ICI-based combination regimens in patients with HCC, highlighting the spectrum of clinical presentation and outcomes.
CASE
Case 1
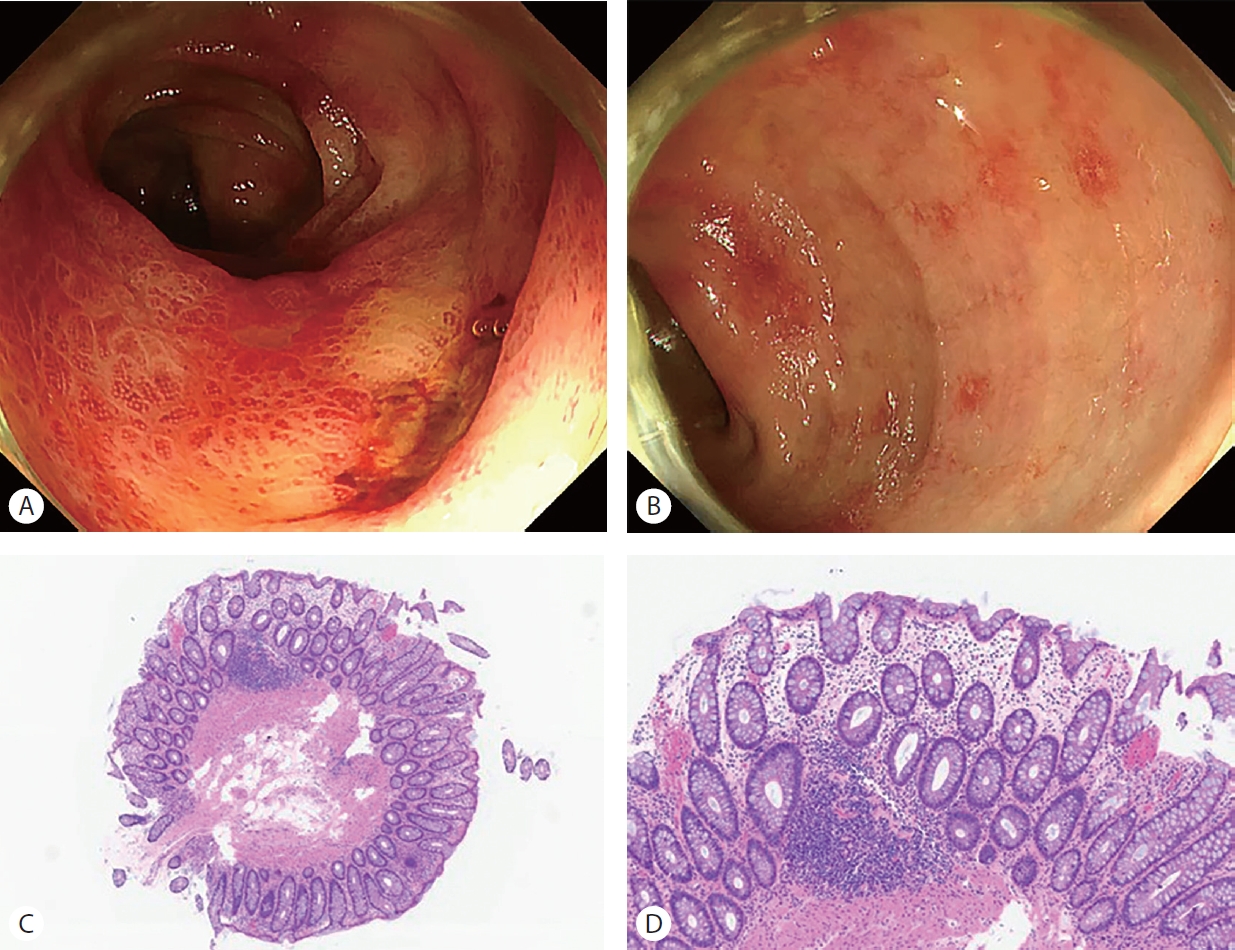
A 70-year-old man was referred to our institution after multiple hepatic masses were incidentally identified on abdominal ultrasonography. Imaging workup and liver biopsy confirmed HCC with multiple bone metastases involving atlas, fifth lumbar vertebra, and left iliac bone, along with a hepatoduodenal ligament lymph node suspicious for metastatic involvement (BCLC stage C). The patient was initiated on the STRIDE regimen (durvalumab 1,500 mg plus tremelimumab 300 mg), concurrently with palliative radiotherapy to the atlas, fifth lumbar vertebra, and left iliac bone (30 Gy in 10 fractions each). Two weeks after the initial durvalumab plus tremelimumab dose, the patient developed CTCAE grade 1 diarrhea (3-4 loose stools per day above baseline, without nausea, abdominal pain, hematochezia, or systemic features). An infectious workup, including stool cultures for enteric pathogens, Clostridioides difficile toxin assay, and stool ova/parasite examination, was negative. Sigmoidoscopy revealed no causative lesion, and random biopsies showed nonspecific chronic inflammation without crypt distortion, neutrophilic cryptitis, or apoptotic bodies, thus not meeting diagnostic criteria for ICI-induced colitis or microscopic colitis. Empirical corticosteroid therapy was considered but was deferred because the symptoms remained grade 1, the histologic findings were nondiagnostic, and current guidelines do not recommend corticosteroids for transient grade 1 diarrhea. Durvalumab monotherapy was therefore administered four weeks after cycle 1. Approximately 90 minutes after the infusion, he developed profuse diaphoresis, diarrhea, vomiting, and dizziness; despite fluid resuscitation, hypotension (blood pressure 75/50 mmHg) and tachycardia (heart rate 139 bpm) persisted, ultimately requiring dual vasopressor support (norepinephrine 1 mcg/kg/min and vasopressin 8 milliunits/min). He subsequently developed metabolic acidosis, oliguria, and respiratory failure necessitating endotracheal intubation with mechanical ventilation and continuous renal replacement therapy (CRRT). Fortunately, he was successfully extubated on day 2 and CRRT was discontinued on day 3. Abdominal computed tomography (CT) revealed diffuse bowel wall thickening with target-like enhancement, and sigmoidoscopy demonstrated multifocal erythema and aphthous ulceration from the descending colon to the rectum. Biopsies of the affected mucosa confirmed chronic inflammation with crypt hyperplasia, consistent with immune-related colitis (
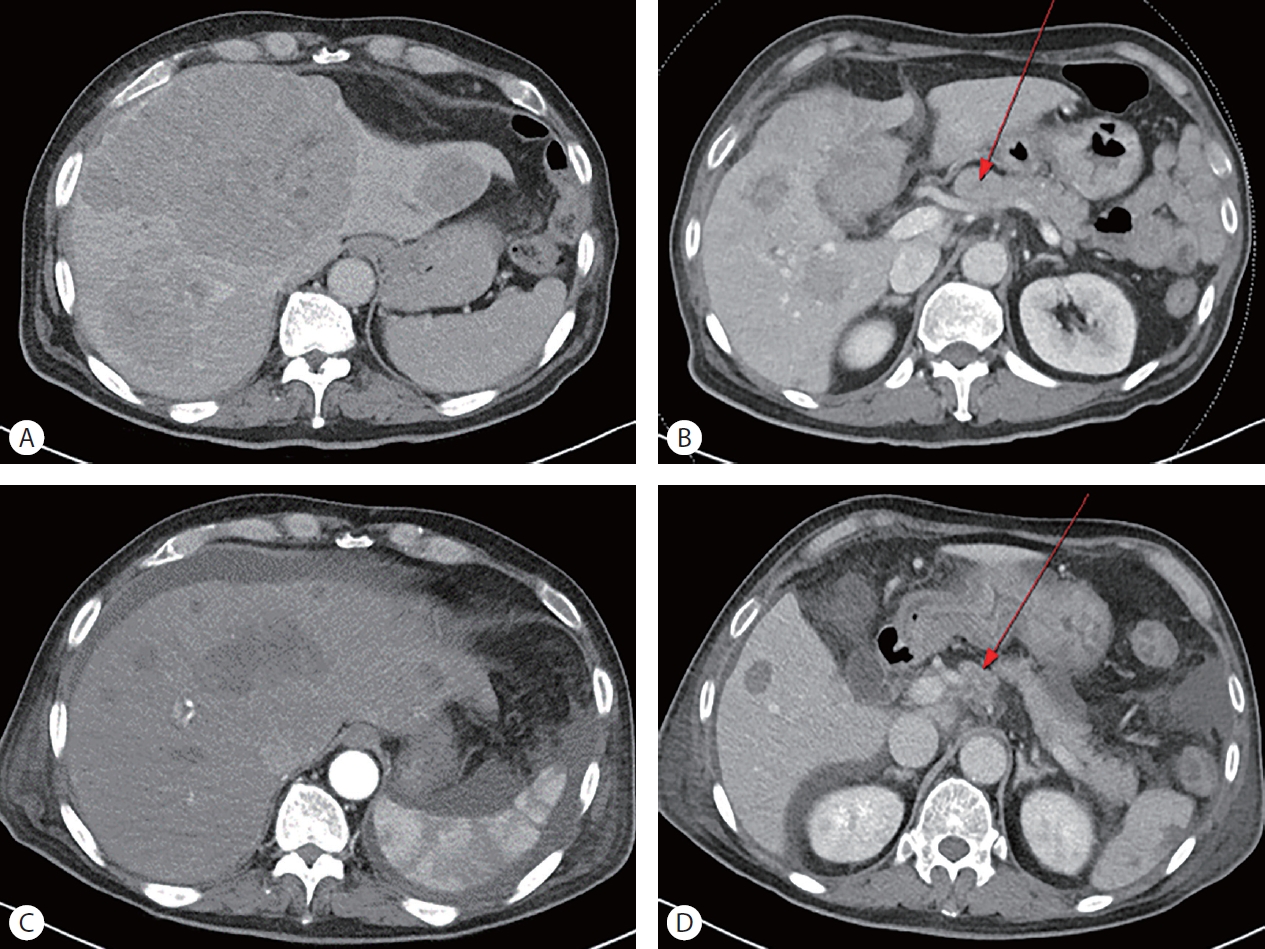
Fig. 1). Compared with pre-treatment imaging, abdominal CT demonstrated a remarkable oncologic response, with complete or near-complete regression of the intrahepatic lesions and regression of the hepatoduodenal lymph node (
Fig. 2). Prior to initiation of corticosteroid therapy, an infectious workup was performed and confirmed negative: stool culture for enteric pathogens (Salmonella, Shigella, Campylobacter), Clostridiodes difficile toxin assay, and stool ova/parasite examination were all negative; serum cytomegalovirus (CMV) PCR was negative, CMV immunohistochemistry on the colonic biopsy specimens demonstrated no cytomegalic inclusion bodies or CMV antigen; and blood cultures showed no growth. Immune-related colitis was then treated with intravenous methylprednisolone 30 mg daily for three days, followed by a gradual oral prednisolone taper over approximately two months (20 mg → 15 mg → 12.5 mg → 10 mg → 7.5 mg → 5 mg), with complete symptomatic resolution.
A 78-Year-old man with hepatitis C virus (HCV)-related liver cirrhosis—who had previously achieved sustained virologic response following interferon based antiviral therapy and had undetectable HCV RNA at the time of HCC diagnosis— was found to have a 1.4-cm Liver Imaging Reporting and Data System category 4 lesion in hepatic segment 4 on magnetic resonance imaging and underwent laparoscopic left hemihepatectomy. Surgical pathology confirmed a 2.0-cm HCC (Edmondson-Steiner predominantly grade III with focal grade II, BCLC stage A). In view of microvascular invasion, the patient was enrolled in the IMbrave050 trial (NCT04102098) [
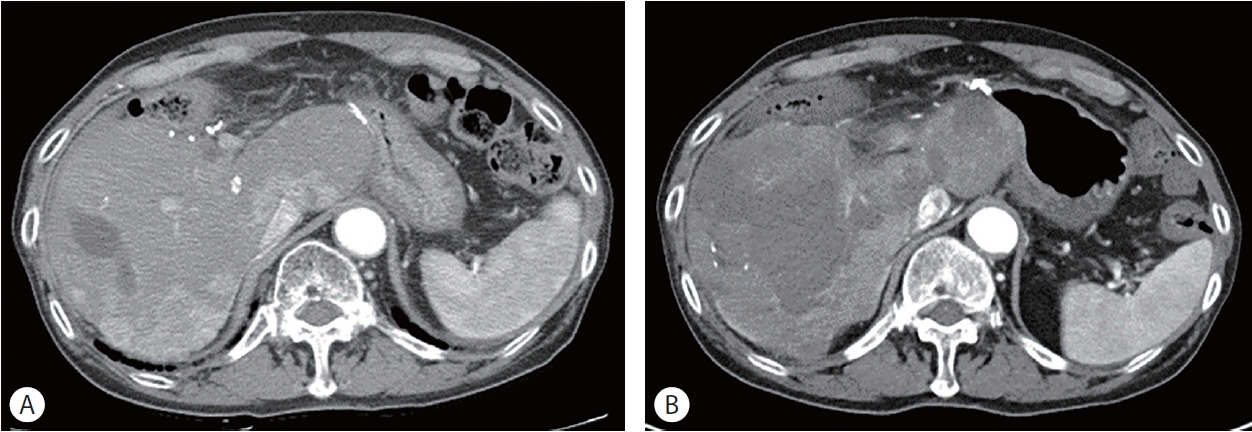
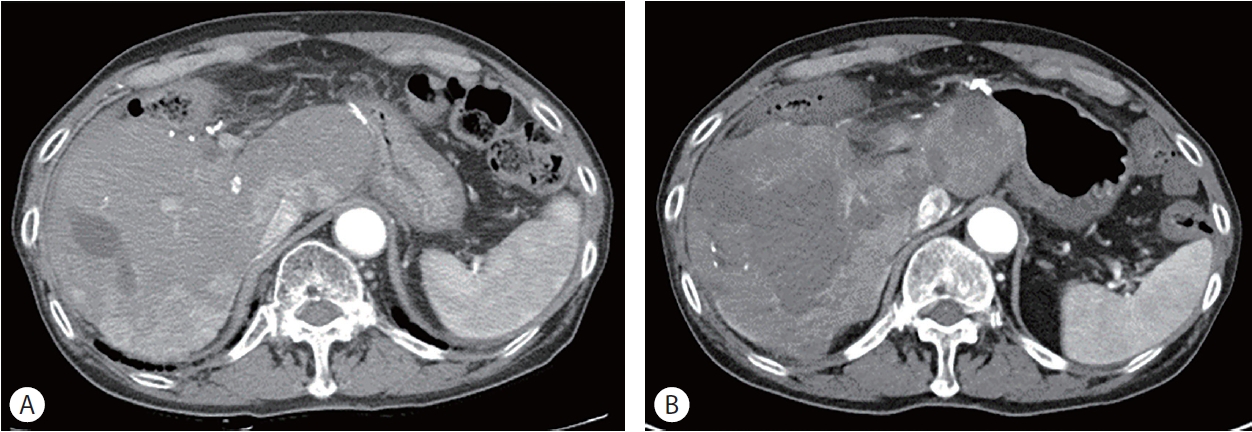
4] and received 17 cycles of adjuvant atezolizumab (1,200 mg) plus bevacizumab (15 mg/kg). At enrollment, the patient was Child-Pugh class A (score 5), ALBI grade 1 (score −2.16), with ECOG performance status 1; HCV RNA remained undetectable throughout the adjuvant course and at the time of subsequent rechallenge. No clinically significant irAE occurred during the 12 months of adjuvant therapy. Despite 12 months of adjuvant therapy, intrahepatic recurrence was documented, and six sessions of transarterial chemoembolization (TACE) were subsequently performed. The patient experienced TACE-related complications including hepatic abscess and bile duct injury with biloma formation. Progressive intrahepatic tumor burden was additionally noted, and the overall course was deemed to represent TACE failure. Approximately two years and ten months after hepatic resection, ate+bev was reinitiated as first-line systemic therapy for unresectable HCC. One week after the first dose of reinitiated ate+bev, the patient was hospitalized with diarrhea, abdominal pain, nausea, vomiting, general weakness, and new-onset dysarthria. Laboratory investigations revealed AST 82 IU/L (baseline 38), ALT 207 IU/L (baseline 26), total bilirubin 1.22 mg/dL (baseline 0.53), INR 1.14 (baseline 1.01), and admission MELD score of 8, and metabolic acidosis. Viral hepatitis was excluded by negative HBsAg, anti-HBc IgM, HBV DNA, HCV RNA, anti-HAV IgM, and unremarkable HEV/CMV/EBV studies. Blood and urine cultures, chest imaging, and procalcitonin did not support an infectious source; the patient was afebrile and normotensive at presentation, and hepatic decompensation preceded both hemodynamic instability and the subsequent variceal hemorrhage, arguing against ischemic or sepsis-related hepatic injury. Baseline contrast-enhanced CT obtained immediately before rechallenge (
Fig. 3A) demonstrated no acute hepatic injury, with stable post-TACE changes and a quiescent biloma; in contrast, follow-up CT after the onset of deterioration (
Fig. 3B) revealed diffuse massive necrosis of the remnant liver in a non-segmental, non-embolization-territory distribution, inconsistent with TACE-related ischemic hepatopathy. The last TACE session had been performed 7 weeks earlier, and the TACE-related complications had been radiologically stable in the preceding months. Liver biopsy was considered but was deferred owing to rapid progressive coagulopathy and active variceal hemorrhage, which precluded both percutaneous and trans-jugular approaches. The constellation of findings— acute massive hepatic necrosis temporally linked to atezolizumab re-exposure, in the absence of viral, ischemic, septic, drug-induced, or TACE-related etiologies—was consistent with CTCAE v5.0 grade 4 immune-mediated fulminant hepatitis. In accordance with ESMO and ASCO recommendations for high-grade ICI-related hepatitis, intravenous methylprednisolone (2 mg/kg/day) was initiated within 72 hours of admission, accompanied by ICU-level supportive care. Because hepatic and synthetic dysfunction continued to worsen despite 24 hours of high-dose corticosteroid therapy, mycophenolate mofetil (2g/day) was added as a second-line immunosuppressant on hospital day 5. As MELD score escalated and multi-organ failure progressed, mechanical ventilation was initiated and continuous renal replacement therapy (CRRT) commenced on hospital day 5. The clinical course was further complicated by upper gastrointestinal bleeding, presumed to be of variceal origin, which was managed with SB tube and pharmacologic therapy. Liver transplantation was considered the only potentially life-saving intervention; however, it was declined by the family, and the patient died 22 days after the first dose of reinitiated ate+bev.
DISCUSSION
These cases highlight the unpredictable nature of irAEs and provide important clinical insights into the management of advanced HCC in the era of ICI-based combination therapies. The onset and presentation of irAEs can deviate substantially from established patterns, and these two cases demonstrate both ends of the clinical spectrum. In Case 1, gastrointestinal toxicity emerging within two weeks of the first STRIDE cycle is broadly consistent with the known predilection of anti-CTLA-4 agents for early gastrointestinal irAEs [
2]; however, the histologically indeterminate findings on initial sigmoidoscopy are atypical and serve as an important reminder that immune-mediated mucosal injury may be subclinical at first presentation—a negative biopsy alone should not preclude continued vigilance. In Case 2, fulminant hepatitis within one week of a single dose of ate+bev represents a far more accelerated onset than the weeks-to-months timeline reported in IMbrave150 [
1]. We hypothesize that subclinical immune priming during the prior adjuvant course persisted across the treatment-free interval, generating an anamnestic recall response upon re-exposure. This mechanism remains speculative and requires confirmation in mechanistic studies; alternative explanations are systematically considered in the paragraphs that follow. Clinicians must therefore maintain heightened vigilance during the initial cycles of any new ICI treatment phase, even in patients with a prior history of tolerability.
Given the immediate post-infusion timing of the hemodynamic collapse in Case 1, an acute infusion-related reaction and cytokine release syndrome (CRS) were considered. However, the absence of fever, urticaria, bronchospasm, or angioedema; the dominance of severe diarrhea and vomiting; the imaging finding of diffuse target-like bowel wall thickening; the multifocal endoscopic ulceration; and the histologic confirmation of crypt hyperplasia with chronic inflammation collectively excluded these alternative entities and supported immune-mediated colitis with diarrhea-driven distributive shock. We acknowledge that an early cytokine-mediated component may have acutely amplified pre-existing subclinical mucosal inflammation; this possibility does not alter the principal therapeutic implication, which is prompt corticosteroid initiation.
An additional consideration in Case 1 is the potential role of concurrent palliative radiotherapy. Radiation can release tumor-associated antigens, upregulate MHC class I expression, induce immunogenic cell death, activate the cGASSTING pathway, and enhance dendritic cell maturation and CD8+ T-cell priming, mechanisms that underlie the abscopal effect observed when radiation is combined with checkpoint blockade. The same mechanisms that potentiate antitumor immunity may also lower the threshold for off-target immune toxicity by expanding activated T-cell clones and amplifying systemic pro-inflammatory signaling. Although the 30-Gy in 10-fraction palliative regimen delivered to three osseous sites is unlikely on its own to have produced the near-complete intrahepatic and nodal regression observed in Case 1, it plausibly functioned as a systemic immune adjuvant that contributed both to the depth of the antitumor response and to the severity of the immune-mediated colitis, consistent with the established correlation between irAE occurrence and treatment efficacy.
The clinical course of Case 2 is, to our knowledge, unprecedented in the published literature. Pharmacovigilance data indicate that the same irAE recurs in approximately 28.8% of patients upon ICI rechallenge, and that hepatitis is among the irAEs most strongly associated with recurrence (reporting odds ratio 3.38, 95% CI 1.31–8.74) [
5]; cohort studies report recurrence rates of 23.5–35% form immune-mediated hepatitis after rechallenging [
6-
8]. Nevertheless, fatal recurrent hepatitis is exceptional, and—critically—the great majority of these reports describe patients who experienced an irAE during the index ICI course and were subsequently rechallenged after recovery. Our patient differs fundamentally: 17 cycles of adjuvant atezolizumab plus bevacizumab were completed without any irAE, and fulminant hepatitis emerged within a single week of reinitiation of the identical regimen as firstline systemic therapy for recurrent disease. This scenario— rechallenge after an uneventful adjuvant ICI course—has, to our knowledge, not previously been described as a cause of fatal immune-mediated hepatitis, and its recognition is important because adjuvant ate+bev is increasingly used in high-risk advanced-stage HCC.
Mechanistically the accelerated and disproportionate hepatic injury observed upon re-exposure is plausibly explained by anamnestic reactivation of memory T-cell populations. ICI therapy induces clonal expansion of activated effector-memory CD4+ and CD8+ T cells and the seeding of tissue-resident memory T (TRM) cells in extralymphoid tissues, including the liver, which can persist for many months after drug discontinuation. Re-exposure to PD-L1 blockade may have triggered rapid recall responses from these primed populations, producing a high-magnitude inflammatory reaction that exceeded the threshold of hepatic tolerance—particularly in a liver with reduced functional reserve due to underlying HCV cirrhosis and recent TACE-related injury. This mechanistic model is concordant with the one-week interval between rechallenge and clinical decompensation in our patient, which is substantially shorter than the median 6–8-week time-toonset of ICI-related hepatitis reported in IMbrave 150 [
9]. The hypothesis nevertheless remains speculative and requires confirmation in mechanistic studies, including longitudinal immunophenotyping and analysis of intrahepatic T-cell clonality in similar cases.
Alternative explanations for the fatal hepatic event in Case 2 were systematically considered and were judged less likely to account for the clinical picture. (i) TACE-related parenchymal and biliary injury, including the previously documented biloma, was radiologically stable for several months before rechallenging, and the baseline contrast-enhanced CT obtained immediately before reinitiation of ate+bev showed no acute injury. (ii) Hepatic abscess was excluded by negative blood cultures, the absence of fever or radiographic abscess, and the lack of leukocytosis. (iii) The pattern of hepatic injury on follow-up CT was diffuse massive remnant-liver necrosis rather than tumor-related parenchymal replacement, arguing against tumor progression as the primary cause. (iv) Ischemic hepatopathy was unlikely given normotension at presentation, a non-territorial imaging pattern, and the development of vasopressor requirement only after the onset of hepatic decompensation. (v) Vascular events including portal venous and hepatic arterial thrombosis were excluded by Doppler ultrasound and contrast-enhanced CT, and bevacizumab-associated thromboembolic events were specifically considered and not identified. (vi) Infectious etiologies, including HBV reactivation, HCV virologic breakthrough, and HAV/HEV/CMV/EBV, were excluded by the corresponding serologic and molecular studies. We nonetheless acknowledge that underlying HCV cirrhosis with reduced hepatic functional reserve and the residual effects of prior TACE-related injury constitute important predisposing factors that likely amplified the severity of the immune-mediated event.
Several features of HCC fundamentally complicate the recognition and management of irAEs compared with other tumor settings, and our two cases collectively illustrate these challenges. First, the great majority of HCC patients have underlying cirrhosis with limited hepatic functional reserve, so even a moderate degree of immune-mediated hepatocellular injury may precipitate hepatic decompensation that disproportionately exceeds the apparent grade of transaminase elevation. Second, irAE hepatitis must be distinguished from a broad differential that is unique to HCC, including viral hepatitis flare or reactivation, TACE- or ablation-related ischemic and biliary injury, tumor-related hepatic decompensation, drug-induced liver injury from concurrent antiviral or supportive medications, and bacterial cholangitis—each requiring a distinct diagnostic and therapeutic response. Third, because patients with HCC frequently receive sequential or combined locoregional and systemic therapies, the temporal attribution of new hepatic injury is often ambiguous, as illustrated in Case 2, where prior TACE-related biliary complications created diagnostic uncertainty that we addressed by detailed exclusion of alternative etiologies, careful temporal correlation, and analysis of the imaging pattern. Fourth, while irAEs of the gastrointestinal tract, endocrine system, and skin in non-HCC populations are usually fully reversible, immune-mediated hepatitis superimposed on cirrhosis in HCC carries an inherently higher case-fatality rate, as exemplified by Case 2. These considerations argue for a low threshold for hepatology consultation in HCC patients receiving ICI-based combination therapy, individualized risk-benefit assessment before any ICI rechallenge in patients with prior hepatic toxicity or with significant pre-existing hepatic compromise, and explicit attention to the possibility of accelerated and amplified hepatic toxicity upon re-exposure, even after previously uneventful adjuvant ICI courses.
The severe colitis followed by a near-complete oncologic response in Case 1 underscores the well-described association between immune-mediated toxicity and treatment efficacy. This phenomenon likely reflects a state of robust systemic T-cell activation in which activated immune effectors simultaneously target tumor antigens and self-antigens. Consistent with this, the HIMALAYA trial demonstrated that patients who experienced irAEs with STRIDE had numerically improved overall survival compared with those who did not (median OS 23.2 vs. 14.1 months; HR 0.73) [
2], suggesting that irAE occurrence may serve as a surrogate marker of effective immune activation.
The distinct toxicity profiles of these two cases reflect the differing mechanisms of their respective regimens. In Case 1, dual CTLA-4 and PD-L1 blockade with STRIDE conferred a predisposition to gastrointestinal toxicity: CTLA-4 inhibition disrupts regulatory T-cell homeostasis in the intestinal mucosa, and even a single priming dose of tremelimumab may initiate subclinical mucosal T-cell dysregulation that may cross the threshold for overt colitis upon subsequent PD-L1 blockade. In Case 2, PD-L1 blockade by atezolizumab targeted the liver’s intrinsic immune tolerance mechanisms—PD-L1 is constitutively expressed on hepatocytes, sinusoidal endothelial cells, and Kupffer cells—while bevacizumab-mediated VEGF inhibition may have further modulated the hepatic immune microenvironment, synergistically amplifying cytotoxic T-cell responses against hepatic parenchyma [
10].
We report two cases of clinically severe irAEs following ICI-based therapy for HCC: immune-mediated colitis with shock that resolved with corticosteroid therapy and was accompanied by a remarkable oncologic response, and immune-mediated fulminant hepatitis that proved fatal despite aggressive immunosuppression, arising after a single dose of reinitiated atezolizumab plus bevacizumab in a patient who had previously tolerated 17 cycles of the same regimen without incident. These cases collectively emphasize that irAEs in HCC are unpredictable in onset and severity, may be exacerbated by prior hepatic compromise, and require prompt multidisciplinary management guided by both organ-specific and patient-specific risk factors.
NOTES
-
ACKNOWLEDGEMENTS
This work was supported by clinical research grant from Pusan National University Hospital in 2024.
-
FUND
This work was supported by clinical research grant from Pusan National University Hospital in 2024.
-
ETHICS STATEMENT
Consent for publication is not required, as this submission does not include any images or information that could identify any individual.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: J Heo. Data curation: HY Woo, J Heo. Writing - original draft: YJ Park. Writing - review & editing: YJ Park, HY Woo. Resources: K Lee. Supervision: HY Woo, J Heo
Figure 1.Endoscopic and histopathologic findings of immune-mediated colitis in Case 1. (A, B) Sigmoidoscopy demonstrating multifocal erythema and aphthous ulceration extending from the descending colon to the rectum. (C, D) Hematoxylin-eosin-stained sections (x4 and x10, respectively) showing increased lymphoplasmacytic infiltration in the lamina propria, crypt hyperplasia, and presence of cryptitis (neutrophilic infiltration of the crypt epithelium) and crypt abscesses. These findings are consistent with ICI-induced colitis.
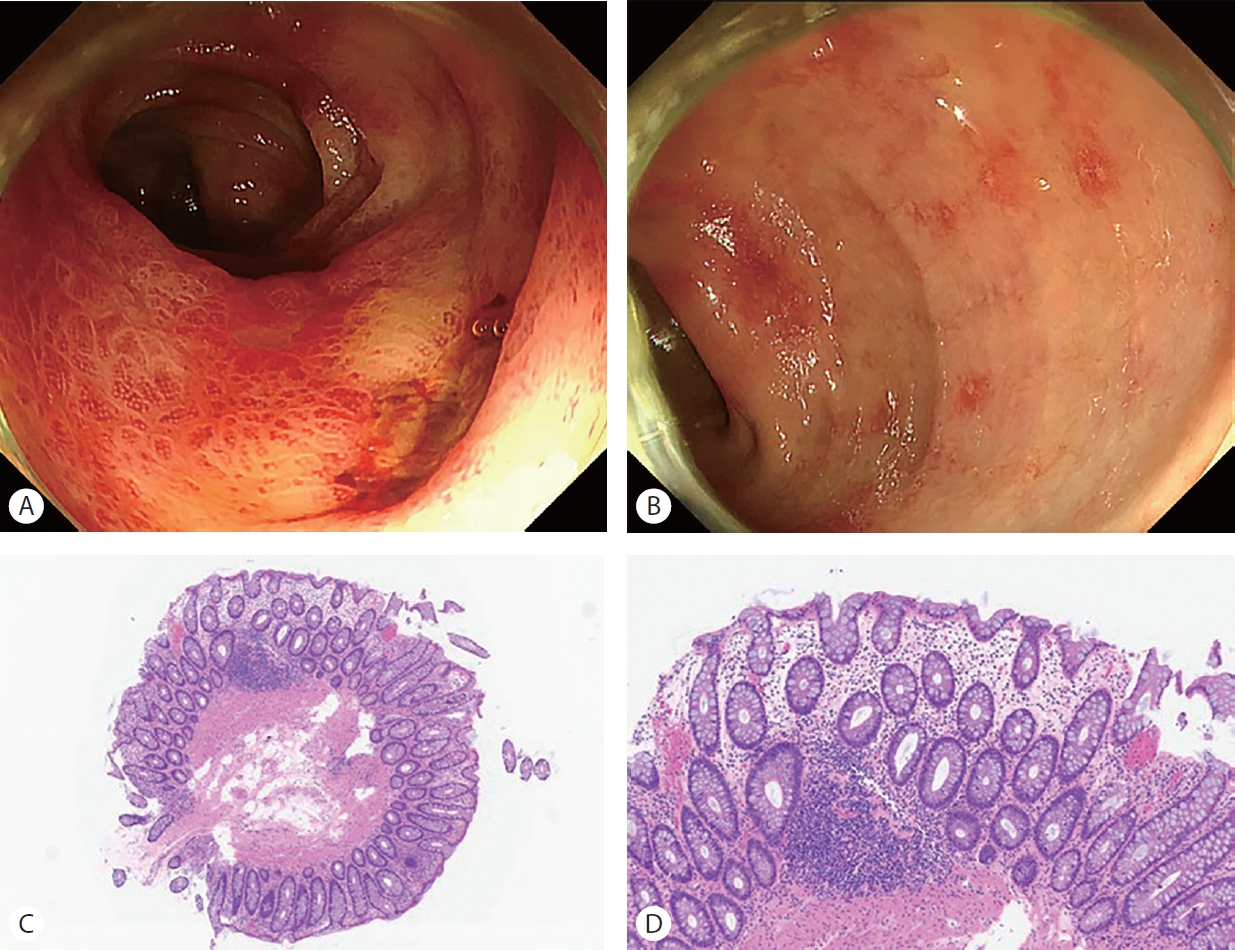
Figure 2.Abdominal CT findings in Case 1 before and after STRIDE treatment. (A) Pre-treatment CT showing multiple hypervascular hepatic masses. (B) Pre-treatment CT demonstrating a suspicious metastatic lymph node in the hepatoduodenal ligament (arrow). (C, D) Follow-up CT obtained approximately 4 weeks after the initial STRIDE cycle, showing (C) complete or near-complete regression of the intrahepatic lesions and (D) interval reduction in size of the hepatoduodenal ligament lymph node (arrow). CT, computed tomography.
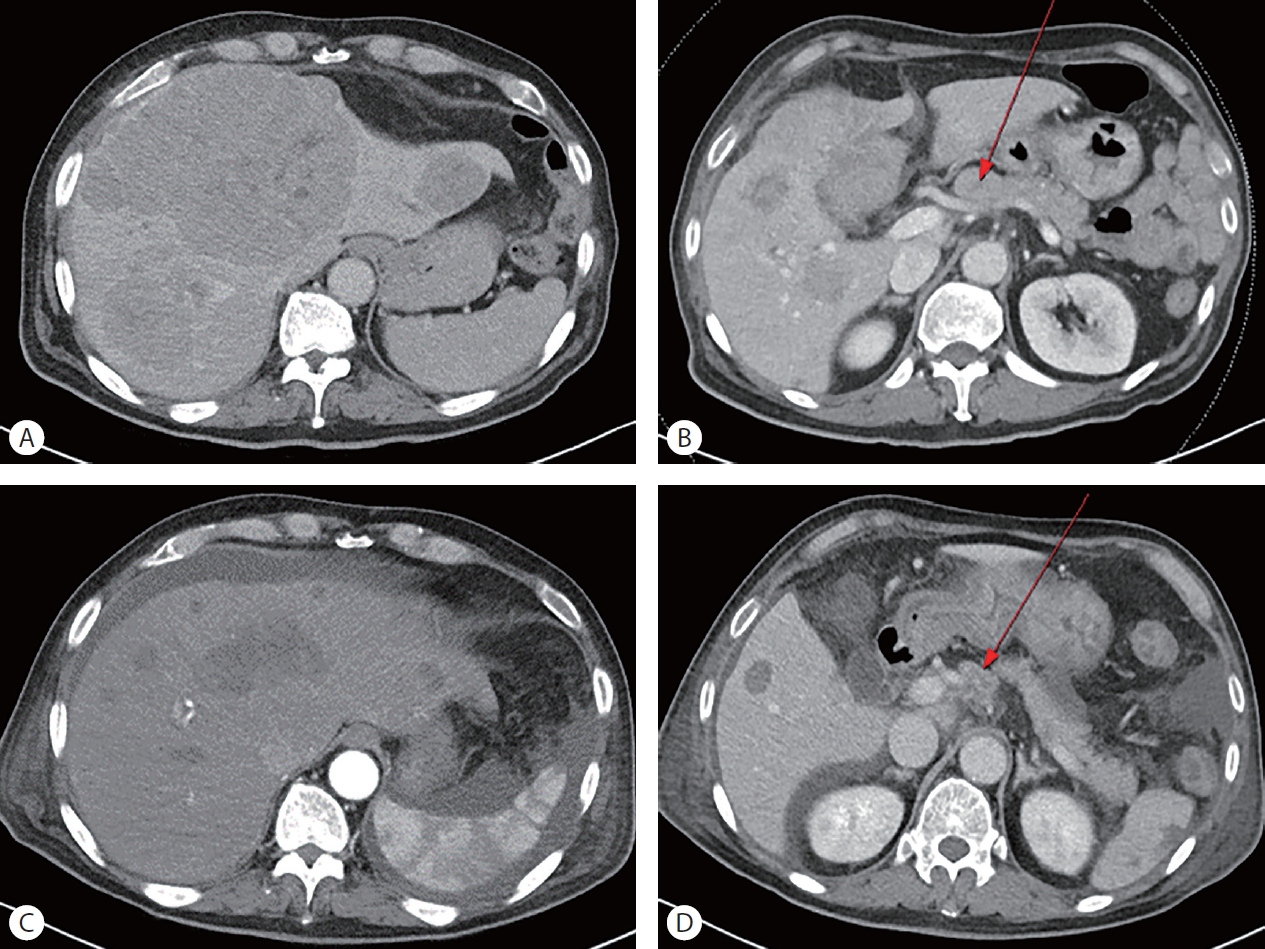
Figure 3.Abdominal CT findings in Case 2. (A) Baseline CT prior to reinitiation of atezolizumab plus bevacizumab, showing the remnant liver following left hemihepatectomy without evidence of acute hepatic injury. (B) Follow-up CT obtained after the onset of clinical deterioration, demonstrating massive necrosis of the remnant liver consistent with immune-related fulminant hepatitis. CT, computed tomography.
REFERENCES
- 1. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med 2020;382:1894-1905.
- 2. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid 2022;1:EVIDoa2100070.
- 3. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med 2018;378:158-168.
- 4. Qin S, Chen M, Cheng AL, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. Lancet 2023;402:1835-1847.
- 5. Dolladille C, Ederhy S, Sassier M, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer. JAMA Oncol 2020;6:865-871.
- 6. Pollack MH, Betof A, Dearden H, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann Oncol 2018;29:250-255.
- 7. Riveiro-Barciela M, Barreira-Díaz A, Callejo-Pérez A, et al. Retreatment with immune checkpoint inhibitors after a severe immune-related hepatitis: results from a prospective multicenter study. Clin Gastroenterol Hepatol 2023;21:732-740.
- 8. Hountondji L, Ferreira De Matos C, Lebossé F, et al. Clinical pattern of checkpoint inhibitor-induced liver injury in a multicentre cohort. JHEP Rep 2023;5:100719.
- 9. Reschke R, Gajewski TF. Tissue-resident memory T cells in immune-related adverse events: friend or foe? Oncoimmunology 2023;12:2197358.
- 10. Liu Z, Zhu Y, Xie H, Zou Z. Immune-mediated hepatitis induced by immune checkpoint inhibitors: Current updates and future perspectives. Front Pharmacol 2023;13:1077468.