ABSTRACT
Liver cancer is among the most prevalent and life-threatening cancers worldwide, with hepatocellular carcinoma and liver metastases contributing significantly to cancer related mortality. Accurate segmentation of liver tumors in abdominal computed tomography and magnetic resonance imaging is crucial for tumor prediction, radiation therapy, and treatment monitoring. In recent years, medical image segmentation has advanced rapidly due to deep learning (DL), particularly convolutional neural networks (CNN) and transformer-based architectures. This paper provides a comprehensive review of DL based liver tumor segmentation methods in abdominal imaging. We examine the evolution from traditional encoder decoder frameworks such as U-Net and V-Net to residual, attention based, and hybrid CNN transformer models, including vision transformers. The review also analyzes performance across publicly available benchmarks, including the Medical Segmentation Decathlon, 3D-IRCADb, CHAOS, and the Liver Tumor Segmentation Challenge, using evaluation metrics such as Dice Similarity Coefficient, Hausdorff Distance, and Intersection over Union. Furthermore, we discuss key challenges including tumor heterogeneity, class imbalance, limited annotated data, and domain adaptation across imaging protocols. Emerging directions such as foundation models, self-supervised learning, federated learning, and clinically deployable AI segmentation systems are also highlighted.
-
KEYWORDS: Liver tumor segmentation; Deep learning; Computed tomography; Magnetic resonance imaging; LiTS challenge
INTRODUCTION
Liver cancer continues to be a major cause of cancer related deaths and has a substantial impact on global health. In 2020, liver cancer afflicted about 905,700 people worldwide and caused about 830,000 deaths. Global statistics show that liver cancer ranks third in terms of death, despite having the sixth-highest cancer diagnosis rate. While rates of liver cancer are declining in East Asian nations, there is a worrying rise in occurrence in many areas, including the USA and some previously low risk European nations [
1].
One of the most important tools for oncologists to diagnose liver cancer is medical imaging [
2]. Liver cancer is frequently diagnosed using a variety of imaging modalities, such as com-puted tomography (CT), magnetic resonance imaging (MRI), Positron Emission Tomography (PET), and ultrasound [
3,
4]. Accurate tumor segmentation is crucial in clinical practice. In order to evaluate whether therapy should be maintained, modified, or stopped, it enables treatment response evaluation using RECIST. Assessments depend on precise measurements of the longest tumor diameter [
5]. Precise segmentation is also essential for planning surgical resection and administering radiation therapy, which guarantees that doses are targeted to the tumor while avoiding nearby healthy tissues [
6].
Accurate identification of liver tumors in abdominal CT and MRI is critical throughout the oncology workflow. Excessive radiation to nearby liver tissue raises the likelihood of radiation induced liver disease and recurrence in those locations, according to earlier research [
7]. Furthermore, some studies have demonstrated a close correlation between improved survival outcomes for patients with liver cancer and changes in tumor size and volume [
8,
9]. However, the variability of liver tumors, characterized by inconsistent density, morphology, and ambiguous tumor boundaries, makes exact segmentation difficult [
10,
11]. Despite improvements, liver tumor segmentation still faces significant challenges and requires continuous refinement using state-of-the-art methods and clinical expertise [
12]. Despite being the standard, manual segmentation by radiologists and clinicians takes a very long time, between 15 and 90 minutes per CT volume, depending on the complexity of the tumor is prone to significant intra and inter-observer variability (reported Dice disagreements of 10–15% for complex lesions), and is not scalable to the large imaging volumes found in contemporary healthcare systems [
13]. To overcome the limitation of manual segmentation,
Fig. 1 demonstrates the AI pipeline for liver cancer diagnosis.
In the 2000s and early 2010s, a lot of research was done on semi-automated techniques such thresholding, watershed transforms, active contours, level set methods, and graph cut algorithms. Although these techniques provided considerable automation, their clinical use was limited by the need for meticulous parameter tweaking, domain knowledge, and significant manual initialization and correction. The watershed moment in medical image segmentation research arrived with the publication of the U-Net architecture by Ronneberger et al. [
14] also in 2015. U-Net’s elegant encoder-decoder design with skip connections, combined with its ability to train effectively on limited annotated medical imaging data, established it as the de facto standard architecture for medical image segmentation and has spawned hundreds of variants and extensions. Segmentation accuracy and resilience were gradually increased by later developments such as 3D volumetric processing (V-Net) [
15], residual connections (ResU-Net) [
16], attention mechanisms (Attention U-Net) [
17], and dense connectivity (DenseU-Net) [
18].
Recent advances in medical image analysis have been made possible by the success of transformer architectures in natural language processing and their adaptation to computer vision (vision transformer, ViT) [
19]. By better capturing longrange spatial dependencies and global context capabilities inherently limited in purely CNN based approaches, hybrid CNN transformer models like TransUNet [
20] and Swin-UNet [
21], as well as fully transformer-based architectures like UNETR [
22] and nnFormer [
23], have shown state-of-the-art performance on liver tumor segmentation benchmarks. A paradigm change toward general purpose, prompt driven segmentation with little task specific fine tuning is promised by the development of large-scale foundation models, such as Meta AI’s Segment Anything Model (SAM) [
24] and its medical applications [
25,
26].
Despite notable advancements in deep learning (DL) for liver tumor segmentation, current reviews are either clinically disconnected, methodologically limited, or have a limited scope. These shortcomings are fully addressed in this study. The following are this work’s main contributions:
Scope & Coverage: The review is the first to encompass all four methodological eras in a single work: foundation models (SAM/MedSAM), CNNs, transformers, and classical approaches.
Structured Tables: We present a comprehensive comparative analysis of liver tumor segmentation methods by summarizing tumor Dice Similarity Coefficient (DSC) values reported from the three categories of techniques: pre–DL methods, CNN-based models, and Transformer based approaches. Tumor DSC refers specifically to the DSC used to evaluate tumor (lesion) segmentation performance.
We further report segmentation performance based on DSC scores on the Liver Tumor Segmentation Challenge (LiTS) dataset benchmark (hereafter referred to as LiTS DSC), a widely used dataset for liver and tumor segmentation evaluation. The values presented in the comparative tables represent approximate median results derived from published studies, and when direct LiTS results were not available, values were estimated from comparable experimental settings or similar benchmarks to maintain consistency in the analysis.
Foundation Models: Specifically, liver tumor standards with validated measurements and diagnostic context are used to assess medical SAM adaptations (MedSAM, SAMMed3D, SegVol).
This paper is organized as follows for the rest of it. Clinical and imaging background is given in Systematic review methodology and study selection. The search strategy and selection criteria are described in Clinical and imaging background. Publicly accessible datasets and assessment measures are reviewed in Datasets and evaluation metrics. Classical and early DL methods are discussed in Classical and pre-DL approaches. CNN-based architectures are surveyed in Convolutional neural network approaches. Transformer-based techniques are reviewed in Transformer-based and hybrid architectures. Prompting and foundation models are covered in Foundation models and promotable segmentation. A comparative analysis is given in Comparative analysis and discussion. Future directions are outlined in Future directions. The paper is concluded in Conclusion.
SYSTEMATIC REVIEW METHODOLOGY AND STUDY SELECTION
Search Strategy
This review uses a two-phase literature coverage strategy to assure systematic rigor for the most current and quickly growing methodological breakthroughs, as well as thorough narrative coverage of the whole historical trajectory of liver tumor segmentation research. Phase 1 employs a systematic search following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [
27], focusing on transformer-based architectures and foundation-model-driven approaches published between January 2020 and December 2025, a period during which these paradigms significantly evolved and matured. In addition, the review incorporates recently emerging segmentation paradigms, including State Space Model and Mamba-based architectures such as U-Mamba [
28], SegMamba [
29], and VM-UNet [
30]; SAM-2-based medical foundation models including Medical SAM 2 [
31] and Segment Anything Model 2 for medical imaging [
32]; as well as diffusion-based segmentation frameworks such as MedSegDiff [
33] and MedSegDiff-V2 [
34].
Phase 2 is a supplementary narrative literature review of classical pre-DL methods and CNN-based architectures identified using systematic citation tracking, benchmark publication hand searching, and reference list screening rather than a date-restricted database search. This two-phase design is justified by the fact that transformer based and foundation model methods represent the most rapidly evolving frontier of liver tumor segmentation research, requiring systematic and repeatable identification; in contrast, classical and CNN-based methods are well established and thoroughly documented in foundational benchmark publications and previous surveys, making structured narrative coverage more appropriate and practically feasible than an exhaustive date-restricted systematic search. Only Phase 1 is covered by the PRISMA flow. The narrative review of the CNN-based and classical approaches found during Phase 2, which are not listed in the PRISMA enumeration.
The PRISMA guidelines, which represent the current international standard for transparent and repeatable systematic review reporting, were strictly followed in conducting this Phase 1 systematic review. PubMed, IEEE Xplore, ScienceDirect, Google Scholar, and Scopus are the five main electronic bibliographic databases where a thorough and organized literature search was carried out. These five databases were chosen in accordance with the multi-database approach used by recent high quality systematic reviews in the field [
35], who based their systematic and bibliometric review on Scopus and Web of Science, focusing on neural network based methods for liver semantic segmentation in CT images; and [
36], who searched PubMed, Web of Science, Scopus, and IEEE Xplore for liver segmentation studies with an emphasis on Dice score evaluation PubMed Central.
The following Boolean search string was applied consistently across title, abstract, and keyword fields of each database: (“liver tumor segmentation” OR “hepatic tumor segmentation” OR “liver lesion segmentation” OR “liver cancer segmentation” OR “HCC segmentation” OR “hepatocellular carcinoma segmentation” OR “liver metastasis segmentation”) AND (“deep learning” OR “convolutional neural network” OR “CNN” OR “U-Net” OR “transformer” OR “vision transformer” OR “segment anything” OR “foundation model” OR “machine learning” OR “image segmentation”) AND (“CT” OR “computed tomography” OR “MRI” OR “magnetic resonance imaging” OR “abdominal imaging”)
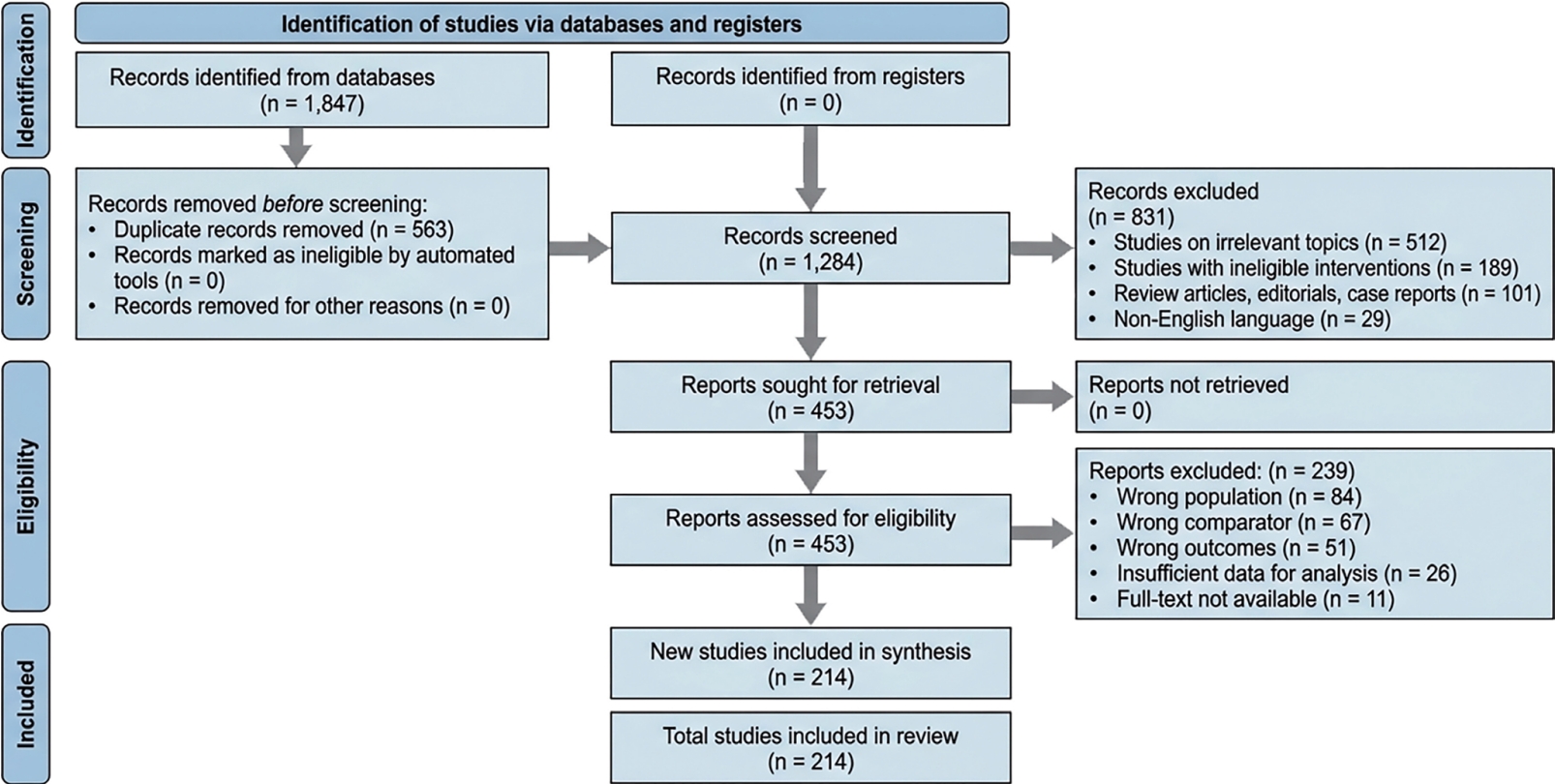
The main search window included articles published between January 2000 and December 2025. The active contour model by [
37], the level-set formulation by [
38], and the graph cut approach by [
39] were also included because of their direct and fundamental relevance to the classical methods reviewed in Classical and pre-DL approaches. Before deduplication, 1,847 records were initially obtained from each of the five databases. After 563 duplicate records from overlapping database coverage were eliminated, 1,284 distinct records moved on to the title and abstract screening stage. A final corpus of 214 studies was kept for inclusion in this evaluation after 453 records underwent full-text eligibility assessment following the methodical application of the inclusion and exclusion criteria outlined in Inclusion criteria and Exclusion criteria. The 214 included research is divided into four methodological eras: 21 foundation model and promptable segmentation studies, 61 transformer-based and hybrid architecture studies, 94 CNN-based DL studies, and 38 pre-DL and classical method investigations.
The PRISMA flow diagram, which shows the processes of study identification, screening, eligibility evaluation, and inclusion, is shown in
Fig. 2. The amount of records excluded at each stage, along with the main causes, are shown in boxes on the right.
Studies that proposed a novel liver tumor or hepatic lesion segmentation method utilizing abdominal CT or MRI and were original, peer-reviewed publications, conference papers, or workshop papers were included. A recognized benchmark dataset (LiTS, MSD, 3D-IRCADb, CHAOS, or SLIVER07) or a private dataset with at least 50 participants had to be used, and the method required to fit into one of four categories: classical/pre-DL, CNN-based, transformer-based, or foundation model approaches. It was necessary to have at least one standard metric (DSC, Intersection over Union [IoU], HD95, Sensitivity, Specificity, or Volumetric Overlap Error. Published between 2000 and 2025, full text in English was required.
Exclusion Criteria
Studies that simply examined liver parenchyma or non-hepatic organs without any tumor segmentation component were disqualified. Regardless of modality, studies that solely addressed tumor detection, classification, diagnosis, staging, or prognosis without voxel-level segmentation were disqualified. Studies with solely qualitative results or non-standard measurements, as well as those with fewer than 20 subjects and no public benchmark validation, were disqualified due to inadequate reliability. Only the more comprehensive version was kept when there were multiple conference and journal versions. Except for SAM-Med2D, SAM-Med3D, and MedSAM, which were included and marked because of their substantial community acceptance, unreviewed preprints with fewer than 100 citations were omitted. Additionally, studies with synthetic only evaluation, totally manual segmentation without any automated component, or inaccessible whole text were not included.
CLINICAL AND IMAGING BACKGROUND
Liver Anatomy
The liver is the largest solid organ in the human body, weighing approximately 1,400-1,600 grams in adults and occupying the right hypochondrium and epigastrium. The human liver is a complicated organ having tiny caudate and quadrate lobes in addition to the two major lobes, the right and left. It collects blood from the portal vein and the hepatic artery, and it drains blood into the inferior vena cava via the hepatic veins. The biliary system, which collects and transports bile produced by liver cells to the duodenum, is part of the internal structure of the liver [
36,
40].
The falciform ligament, which, together with the coronary ligaments, secures the liver to the abdominal wall and diaphragm, divides it externally into the bigger right lobe and smaller left lobe. The liver has a special dual blood supply at the portal triad, where oxygenated blood from the hepatic artery and nutrient rich blood from the hepatic portal vein reach the organ simultaneously. The hepatic lobule is a hexagon shaped functional unit where blood filters through sinusoids lined with hepatocytes. These cells carry out vital metabolic functions and generate bile, which enters bile canaliculi in the opposite direction of blood. Following collection through the hepatic ducts, this bile is either sent through the common bile duct for digestion in the small intestine or transferred via the cystic duct for storage in the gallbladder. The central veins, which eventually unite with the hepatic veins and empty into the inferior vena cava to return to systemic circulation, are the final route by which filtered blood leaves the lobules.
Imaging Modalities
Due to its high spatial resolution and contrast qualities, CT and MRI is still the most widely used imaging modality for liver analysis. However, other imaging modalities, such as ultrasound, and PET, offer alternative approaches with distinct benefits and drawbacks.
CT provides anatomic information about various tissue types by rotating an X-ray tube [
41]. MRI offers better soft-tissue contrast than CT scans. This is especially useful for detecting liver abnormalities, identifying tumors, and distinguishing between benign and malignant developments. Advanced MRI sequences, including pre- and postcontrast T1-weighted imaging, T2-weighted imaging, and diffusion-weighted imaging, provide a thorough study of liver tissue [
42]. Both CT and MRI usually produce three-dimensional (3D) images, but we can also obtain four-dimensional (4D) data by recording their dynamic sequence.
Ultrasound is a widely accessible and reasonably priced imaging modality that is essential for liver evaluation. By offering real-time perfusion imaging, contrast-enhanced ultrasonography (CEUS) enhances the visibility of hepatic lesions [
43,
44]. PET imaging offers functional and metabolic insights into liver cancers, especially when paired with CT (PET/CT). The main purposes of PET/CT are to stage liver cancers, identify metastases, and evaluate the effectiveness of treatment [
45,
46].
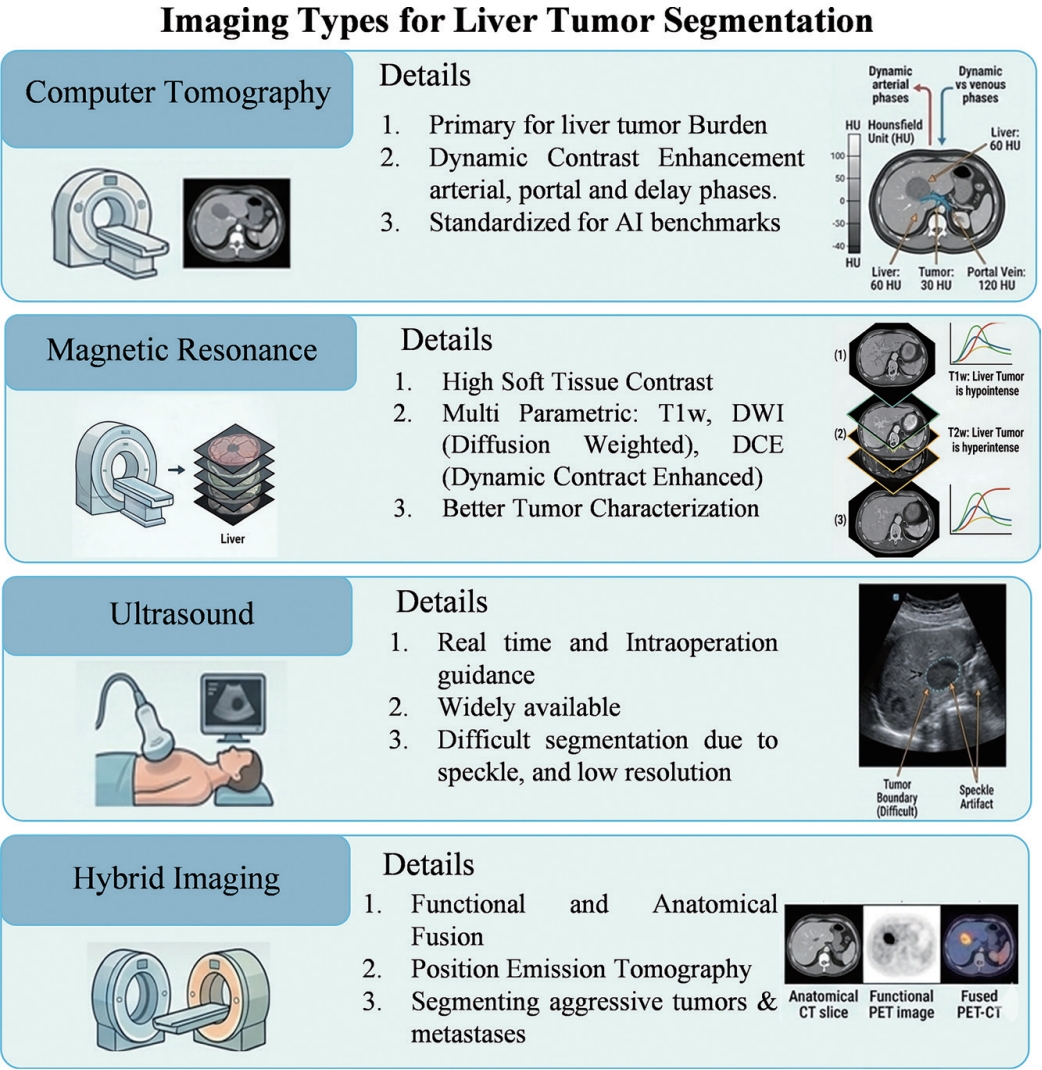
Fig. 3 provides a comprehensive overview of the primary multimodal imaging techniques used in clinical practice for liver tumor segmentation, highlighting the unique physical principles, diagnostic strengths, and specific limitations of CT, MRI, Ultrasound, CEUS, and hybrid imaging (PET-CT/MRI). We focus on CT and MRI modalities for liver tumor analysis:
Clinical relevance and widespread use: CT and MRI are the most widely used imaging modalities for liver tumor diagnosis, staging, and treatment planning, making research based on these modalities directly applicable to real clinical practice.
Complementary imaging characteristics: CT provides detailed anatomical structures, while MRI offers superior soft tissue contrast, enabling better characterization and delineation of liver tumors.
Availability of benchmark datasets: Most publicly available and well annotated liver tumor segmentation datasets are based on CT and MRI, allowing reliable training, validation, and fair comparison with existing state-of-the-art methods.
Clinical Significance of Accurate Segmentation
Compared to conventional methods [
47], high-precision liver segmentation greatly improves diagnostic accuracy, facilitating disease identification, functional assessment, and treatment planning [
48,
49]. It also reduces manual errors and time consumption. Its smooth integration into computer-aided diagnosis (CAD) systems increases productivity and reduces the workload of radiologists [
49,
50]. Lightweight models allow real time applications, even in settings with limited resources [
49,
51]. Cross-modality models further improve segmentation accuracy and are compatible with multiple imaging modalities, such as CT, MRI, and ultrasound, supporting a variety of clinical applications, including diagnosis, surgical planning, and monitoring [
52]. It is essential for both therapeutic and surgical applications, supporting image guided surgeries, 3D liver reconstruction, and preoperative planning [
47,
53], radiation therapy planning, and precise liver volumetry for selective internal radiation therapy [
52,
54]. The technique successfully manages both pathological and healthy livers, including cases with low contrast and blurred edges [
48,
55]. However, there are still issues with segmenting lesions and atypical anatomies, which call for additional improvements [
56]. While label-efficient models lessen dependency on annotated datasets, enhancing practicality [
57], automation eliminates the need for manual segmentation, guaranteeing consistency and repeatability [
58]. Although earlier models from 2015 laid the groundwork despite computational constraints [
59,
60], broader clinical use necessitates validation on larger and more diverse datasets to improve generalizability [
61].
DATASETS AND EVALUATION METRICS
Publicly Available Datasets
The development of liver tumor segmentation has been greatly aided by the availability of big, excellent, openly annotated datasets. The main datasets used in the field are summarized in
Table 1.
The most well-known benchmark is the LiTS challenge [
62], which offers 201 abdominal contrast-enhanced CT volumes with manual annotations for the tumor and liver areas. LiTS is still the most widely used dataset in the reviewed literature. It was designed to address challenges, including diverse lesion types and tissue signals, in chronic liver disease. Comparably, the 3D Image Reconstruction for Comparison of Algorithm Database (3D-IRCADb) [
63] is a well known resource that provides high quality masks for the liver, malignancies, and vascular architecture from 20 to 22 patient scans. Despite the fact that 3D-IRCADb is prized for its intricate 3D reconstructions, the variety of case types that can be used for training may be limited by its small sample size.
The Segmentation of the Liver (SLIVER07) dataset [
64], which includes CT scans of lesions livers and has been widely used for almost 20 years to assess algorithm correctness, is another fundamental resource. However, because it is an older dataset, it could not have the most recent lesion kinds or technologically advanced photos available in more recent collections. The Combined Healthy Abdominal Organ Segmentation (CHAOS) dataset [
65] offers 3D images from 80 patients in both CT and MRI formats to meet the demand for multimodal research. Although CHAOS encourages cross-modality imaging research, its application for disease-specific pathology detection may be limited by its emphasis on healthy organs.
In order to increase model generalizability, the area has recently moved toward comprehensive and large scale benchmarks. Hundreds of contrast-enhanced CT scans from various international clinical facilities are available in the Medical Segmentation Decathlon (MSD) subset for the liver and hepatic arteries. Liver Vessel Segmentation, which consists of 532 CT scans with vessel labels confirmed by top medical specialists, is one example of a specialized dataset for fine-scale structures. Researchers use the ATLAS dataset [
66] for inoperable HCC on contrast-enhanced MRI for unusual diseases and treatment planning.
The underrepresentation of small lesions (less than 1 cm), uncommon tumor subtypes, and populations from low and middle income countries is a significant constraint across the majority of available datasets. Additionally, compared to CT, MRI-based tumor segmentation datasets are still rare, which restricts the creation and verification of MRI-specific algorithms.
Significant obstacles still exist despite these developments, such as the lack of data for uncommon diseases, class imbalance in small structure segmentation, and substantial inter-observer variability in manual annotations. The majority of recent research uses retrospective data from individual centers, which may result in overfitting and selection bias. The development of large, multi-institutional datasets such as AbdomenCT-1K [
56] (1,112 scans), FLARE (2,300 scans), and TotalSegmentator [
67] (1,204 scans for 104 structures), as well as the application of synthetic data generation and SAM to overcome current data limitations, are anticipated to drive future advancements in the field.
The performance of the proposed segmentation method is evaluated in a quantitative manner using standard metrics such as DSC, IoU, and HD. The evaluation measures and benchmark datasets used for liver segmentation performance evaluation are covered in this section.
To measure the effectiveness of liver segmentation algorithms, a number of evaluation metrics have been frequently used. These metrics offer numerical assessments of the degree of agreement between the ground truth annotations and the anticipated segmentation.
Table 2 summarizes evaluation metrics.
Dice Similarity Coefficient: A popular statistic that assesses the degree of overlap between the ground truth and expected segmentation outcomes is the DSC. It calculates the ratio of twice their intersection to the total of the volumes of the segmented region and ground truth region. Better segmentation accuracy is indicated by a high DSC value.
Jaccard Index: Another well-known statistic that determines how comparable the predicted segmentation and ground truth segmentation are is the Jaccard Index, also known as the IoU. It is calculated as the ratio of their junction area to the two areas’ union area. Better segmentation performance is indicated by a higher Jaccard Index.
Sensitivity and Specificity: While specificity (true negative rate) measures the percentage of true negative pixels correctly identified as non liver tumor, sensitivity (also known as recall or true positive rate) measures the percentage of true positive pixels correctly identified as liver. These metrics give information about how well the system can identify liver pixels and filter out non-liver pixels.
Hausdorff Distance: The HD calculates the greatest separation between segmentations of the ground truth and the anticipated region. It indicates the correctness of the segmentation boundary by quantifying the biggest geographic difference between the two sections.
Average Surface Distance: The average distance between the ground truth segmentation boundaries and the predicted segmentation is determined by the average surface distance. The Euclidean distance between the regions is used to calculate it. By measuring the average boundary deviation, it offers a gauge of the overall segmentation accuracy.
Relative Volume Difference: One metric used to quantify the volume difference between the segmented region and the ground truth region is the relative volume difference. It is computed by comparing the segmented volume to the reference volume and is given as a percentage. A perfect match is shown by an RVD value of 0, overestimation is suggested by positive values, and underestimating is indicated by negative values.
Maximum Surface Distance: The maximum distance between the surfaces of the segmented region and the reference region is measured by the Maximum Surface Distance (Max-SD). Better surface matching accuracy is indicated by lower ASD and MSDe values.
Volumetric Similarity: The Volumetric Similarity statistic evaluates how close the actual segmentations and the expected region are in terms of volume. It gauges the algorithm’s accuracy in estimating the liver size by calculating the percentage difference between the volumes of the two regions.
CLASSICAL AND PRE-DL APPROACHES
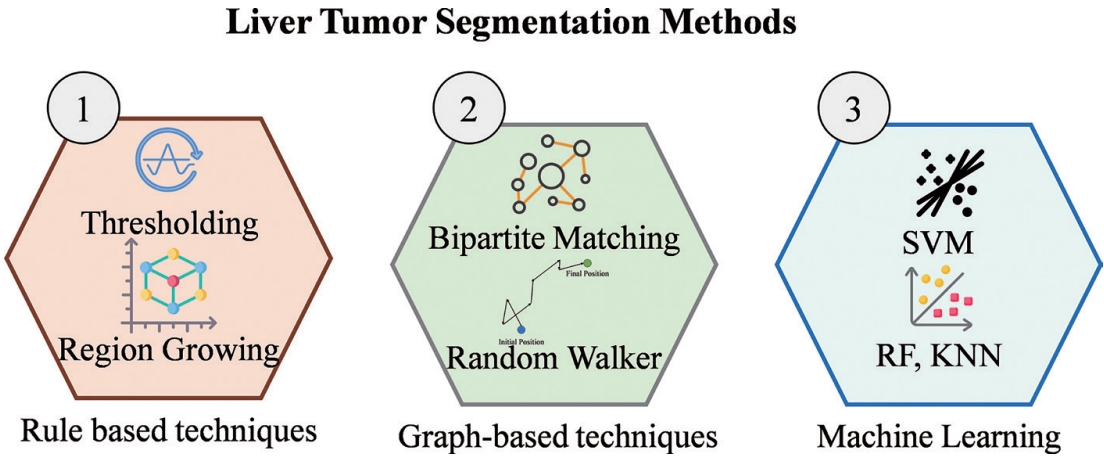
Liver and tumor segmentation relied mostly on manual delineations or semi-automated techniques based on hand-crafted rules and low-level image features prior to the broad use of DL as presented in
Table 3. Conventional methods can be broadly divided into three categories: rulebased image processing techniques, graph-based methods, and classical ML models that use hand-crafted features.
Fig. 4 provides an overview of the primary methodologies used for conventional liver segmentation.
Previous techniques for liver tumor segmentation relied mostly on manually created criteria and low-level image characteristics including intensity, gradients, and edge profiles. Many methods have been used, including thresholding [
68], region growing [
69,
70], edge detection [
71,
72], morphological operations, and active contours (snakes). Although these techniques are easily understood and computationally efficient, they usually struggle with generalization across various imaging modalities and patient populations [
73] and lack robustness when handling noisy data, low contrast boundaries, or significant anatomical variability. In complex clinical circumstances, their dependence on preset heuristics frequently results in subpar performance.
By seeing the image as a network of nodes, graph-based methods most notably Graph Cuts were extensively investigated to produce optimal segmentation solutions. Although these techniques were known to be computationally costly, they frequently coupled shape and enhancement constraints to segment tumors [
74]. In order to improve preliminary rough segmentations, some methods combined them with previous probability maps [
75].
Clinical decision support systems use a variety of data mining and machine learning (ML) techniques to improve the quality of medical judgments and reduce diagnostic errors. In particular, many studies employ ML models to forecast chronic hepatitis B using clinical data. For better liver cancer prediction, the most popular ML algorithms include Logistic Regression (LR) [
76,
77], Decision Tree (DCT) [
78], Random Forest (RF) [
79,
80], and Extreme Gradient Boosting (XGBoost) [
81,
82]. Semantic segmentation uses pixel-wise classification, which produces better classification outcomes by giving each pixel in an image a medical image category label [
35,
83]. The majority of current research in computer image analysis of tissue samples relies on supervised techniques, where ground truth is rarely available for individual tiles and only for the slide as a whole. Furthermore, a significant obstacle to many supervised AI methods in clinical settings has been the implementation of a full annotation [
84].
These approaches had three main clinical challenges, regardless of their great interpretability and effective performance with little datasets. First, they were highly sensitive to noise and imaging aberrations; in CT and MRI scans, the low contrast between tumors and healthy liver parenchyma frequently resulted in “leaking” borders or oversegmentation [
85]. Second, the process was time consuming and susceptible to inter-observer variability because many of these methods were semi-automatic and required extensive manual involvement, such as setting exact seed locations or initializing contours. Finally, because these techniques relied on hand-crafted features and fixed heuristics, they had weak generalizability. The wide morphological heterogeneity in liver morphologies and clinical states across various patient populations and imaging methods was often overlooked by these algorithms.
CONVOLUTIONAL NEURAL NETWORK APPROACHES
In recent years, DL, a branch of ML, has gained significant attention [
86]. CNNs, in particular, have been widely applied to improve liver tumor identification in medical imaging [
87,
88]. CNNs were developed to address the drawbacks of conventional ML techniques by allowing automatic feature extraction using convolutional operations [
89]. CNNs have revolutionized the field of segmenting organs from medical images, particularly in the context of segmenting the liver. CNNs are designed to automatically learn hierarchical representations of input images by employing convolutional layers. These layers perform local operations, capturing spatial features such as edges, textures, and shapes. Through multiple convolutional and pooling layers, CNNs can extract increasingly abstract features, enabling accurate liver tumor segmentation.
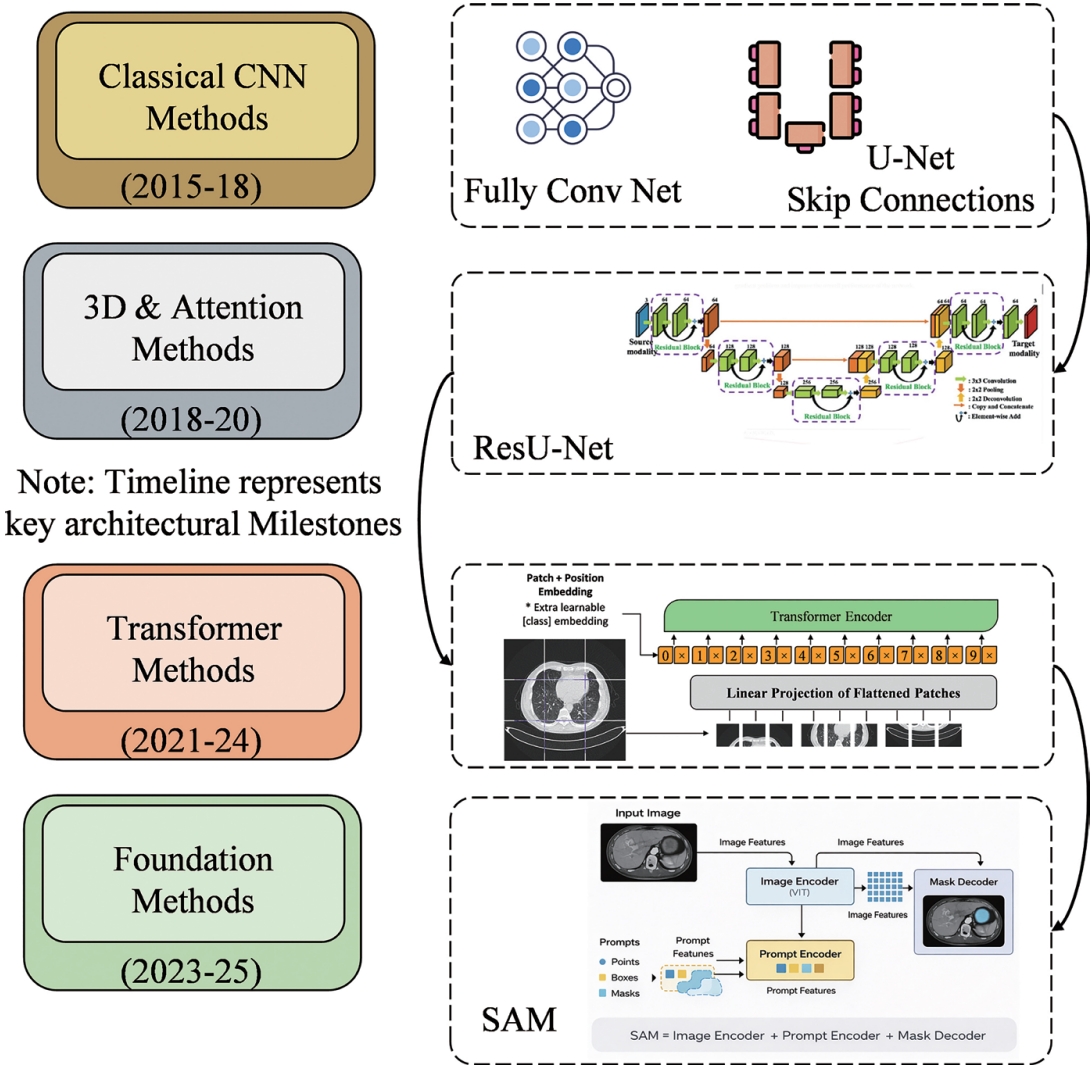
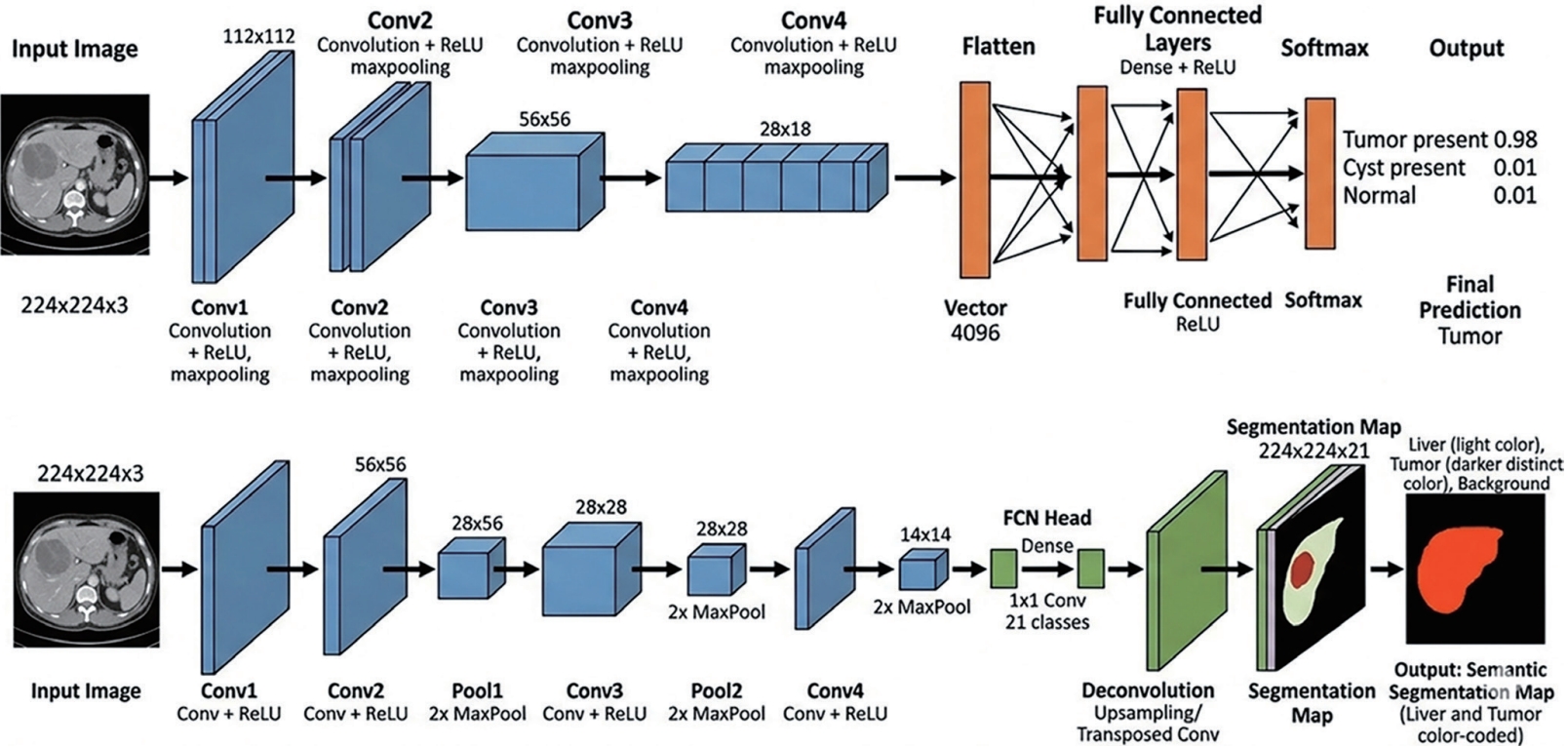
Fig. 5 provides an in-depth visual timeline illustrating the structural development and key innovations in medical image segmentation models from 2015 to the present day.
A significant advancement in image segmentation technology was made in 2015 when suggested Fully Convolutional Network (FCNs) for image segmentation [
90]. Input, convolution, pooling, and output make up its fundamental structure. The fundamental concept of FCN is to substitute the convolutional layer for the fully connected layer at the end of the conventional CNN. The convolutional layer and the pooling layer make up the majority of the network. Any size of input image can be used by the FCN to create an output image that is the same size as the input image. The resnet+FCN network’s skip connection topology makes it easier to restore the network’s whole spatial resolution. It allows for accurate and thorough segmentation by combining semantic information from deeper, coarser layers with the appearance details from shallower, more granular layers. This method extends classification from the image to the pixel level by producing a label prediction for each pixel while maintaining the spatial information of the original input image. It then uses abstract features to restore the category of each pixel in the sampled feature image. There are pre-trained FCN models that can be adjusted for particular tasks (e.g., employing architectures like VGG, ResNet, or MobileNet). FCN is also one of the most commonly used DL architectures, applied for liver and tumor segmentation from volumetric images [
91,
92].
Fig. 6 briefly introduces the algorithms of CNN and FCN.
In 2015, Ronneberger et al. [
14] unveiled the U-Net network. It is an expanded and modified version of the FCN network, and like FCN, U-Net lacks a fully-connected layer. Instead, its network structure is made up of encoders and decoders, and its primary components are the pooling and convolutional layers. The middle skip connection and the left encoder portion make up the majority of the network. The input image’s characteristics are extracted layer by layer by the encoder, while the image’s information is restored layer by layer by the decoder. To increase segmentation accuracy, the middle skip connection combines the lower layer data in the encoder structure with the upper layer data in the decoder structure. The U-Net network is based on the FCN concept, but it learns more effectively and uses less labeled data by adding additional channels, allowing the network’s context information to flow to higher resolution layers, and substituting the upsampling operation for the pooling operation.
In 2018, Zhou et al. [
93] suggested U-Net++ and enhanced U-net. The U-net network structure’s middle skip connection component is the improvement. In order to increase the connectivity between the encoder and decoder sub-networks and decrease the semantic gap between their feature mapping, U-Net++ employs a type of densely connected skip connection that overlays features from several layers.
In 2020, Huang et al. [
94] suggested U-Net3+. To solve these issues, U-Net3+ employs deep supervision and full-scale skip connection. Deep supervision learns feature representations using completely aggregated feature mappings, whereas fullscale skip connectivity integrates high-level semantics with low-level information from features at various scales. In addition to improving segmentation outcomes, the network parameters are reduced and computational efficiency is raised.
Çiçek et al. [
95] proposed 3DU-Net, 3DU-net is an extension of the classic U-net framework which enables 3D volume segmentation. All 2D operations are replaced with corresponding 3D operations, that is, 3D con volution, 3D maxpooling, and so forth, to obtain a three-dimensional segmented image. U-Net++ and U-Net 3+ have been actively applied in liver and liver segmentation.
In terms of applications, Li et al. [
96] suggested the H-DenseUNet, a U-Net variant model, for the segmentation of CT images of the liver and liver tumors. DenseNet-169 is used in this model to extract features from images. A 2D DenseUNet model that effectively extracts feature information from images and a 3D DenseUNet model that aggregates contextual information across polymer elements make up the H-DenseUNet. The H-DenseUNet accomplishes correct segmentation by efficiently extracting 3D feature information from the liver and liver tumor regions.
Residual networks, which were first used in ResNet [
16], are very useful for deep medical image segmentation applications because they improve feature propagation and reduce vanishing gradient problems. ResU-Net and its variations provide deeper networks with better feature reuse by substituting residual blocks for conventional convolutional blocks in U-Net. It has been demonstrated that residual connections speed up convergence, enhance gradient flow in deep architectures, and make it possible to employ pre-trained ResNet encoders as strong transfer learning backbones.
Originally shown in DenseNet [
97], dense blocks improve gradient flow, feature propagation, and parameter efficiency by creating direct connections between all layers in a network stage. Each layer in a dense block reduces duplication and enhances segmentation efficiency by passing its own feature maps forward after receiving input from all layers that came before it. Dense U-Net variations achieved better results on liver segmentation benchmarks by applying DenseNet blocks within the encoder-decoder framework. Dense connection, however, significantly raises memory needs, and volumetric liver segmentation frequently requires memory-efficient variations (e.g., using half-precision calculation and gradient checkpointing). Liver segmentation pipelines incorporated multi-scale feature aggregation modules, such DeepLab’s Atrous Spatial Pyramid Pooling, to simultaneously capture features at several sizes. VM UNet [
30] is a Mamba-based U-Net architecture designed to capture long-range spatial dependencies for efficient and accurate medical image segmentation.
CNN-based methods, anchored by the U-Net encoder-decoder architecture with skip connections, transformed liver tumor segmentation from 2015 onward. Key innovations progressed from 2D slice-based processing through 3D volumetric networks, residual and dense connectivity, multi-scale feature extraction, attention mechanisms, and ultimately the self-configuring nnU-Net framework.
Table 4 compares CNNbased architectures across dimensionality, loss function, key architectural feature, tumor DSC, and LiTS benchmark performance.
The idea behind attention mechanisms is to mimic the human visual system by dynamically weighting in or out particular data points [
98]. The attention mechanism for image processing is based on two principles: a) it can learn a weighted mathematical representation of the inputs that is convolutional-free, allowing focuses or rejection of specific parts of the input data; b) it can model long-distance dependencies by decomposing the image as multiple patches, i.e., ViT implementation [
98]. Channel attention, spatial attention, and hybrid attention (i.e., combining multiple types of attention mechanisms), are the three categories into which attention processes fall. In order to adaptively adjust feature responses, liver segmentation encoders have frequently incorporated channel-wise attention (SE-UNet) [
99] and spatial attention (CBAM-UNet) [
100]. Compared to single scale variations, multi scale attention mechanisms that aggregate attention over various resolution levels have demonstrated gains. As a precursor to the transformer self-attention mechanism, non-local means attention, which was inspired by the classical non-local means filter, calculates attention weights based on feature similarity throughout the whole spatial extent of the feature map [
19]. This effectively captures long range dependencies that local convolutional operations.
TRANSFORMER-BASED AND HYBRID ARCHITECTURES
Originally designed for natural language processing [
101], transformers have been modified for medical image segmentation, including liver segmentation. Transformers gather global contextual information by using self-attention techniques. Transformers take into account the relationships between every pixel in the image, in contrast to CNNs, which rely on local convolutions. Transformers can model intricate pixel interconnections and increase segmentation accuracy thanks to their capacity to encapsulate distant connections. Transformers can efficiently partition the liver and capture fine details by focusing on useful areas in the input image. Transformers have demonstrated promise in improving liver segmentation model performance, especially in situations when global context is important [
19].
Study [
19] proposed the ViT, which modified transformers for image recognition by splitting images into fixed-size patches, embedding each patch linearly, and then using standard transformer encoders to analyze the resulting series of patch embeddings. ViT, which was trained on extensive datasets, demonstrated the effectiveness of self-attention for visual identification by matching or outperforming CNNs on image classification benchmarks.
There were a number of difficulties while using transformers for medical image segmentation. Full-resolution analysis of 3D medical volumes is computationally unfeasible due to the quadratic difficulty of self-attention with respect to sequence length. Annotated medical imaging data is naturally hard to come by, and transformers need huge training datasets to develop efficient representations from start. Pre-training on massive natural image datasets is necessary to make up for the absence of convolutional inductive biases (local connection, translation equivariance) that help CNNs in low-data regimes.
Hybrid CNN-Transformer Models
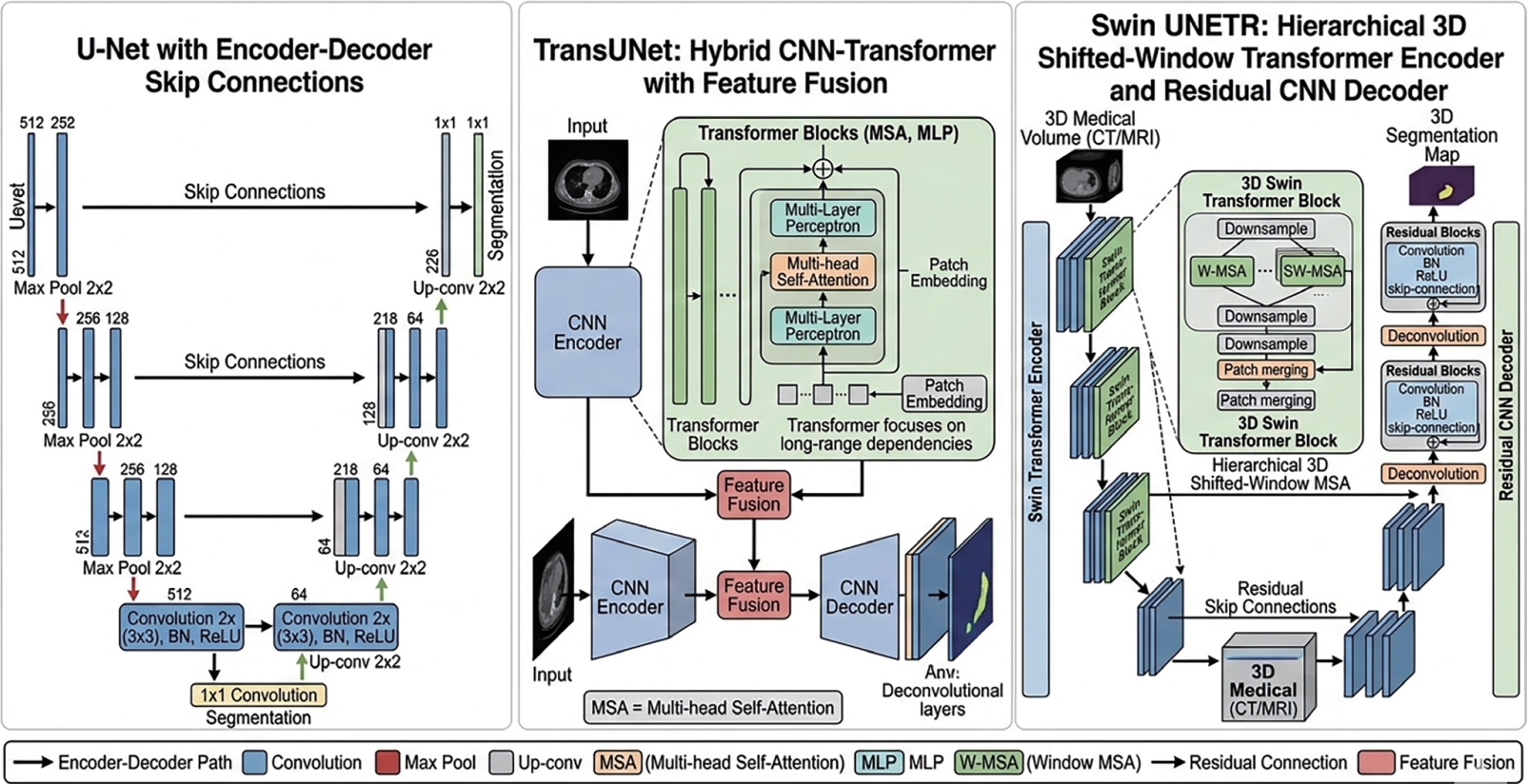
The hybrid CNN-transformer method for medical image segmentation was invented by TransUNet [
20]. It employs a CNN decoder with skip connections after a ResNet-50 encoder with a transformer module added at the bottleneck to collect global context. While the transformer treats the bottleneck feature map as a series of patches to capture long-range relationships, the CNN encoder offers spatially precise local features. TransUNet outperformed U-Net on benchmarks for liver and organ segmentation, confirming the complementarity of CNN and transformer representations.
TranBTS110 [
102] is an effective combination of 3DCNN and Transformer for the multimodal brain tumor segmentation problem in MRI. It uses Transformer to learn global semantic associations while simultaneously utilizing 3DCNN’s capability in modeling local context.
Similar to the U-Net design, Swin-UNet [
21] is the first pure Transformer with a U-shaped encoder-decoder structure with skip connections that uses the decoder to restore the feature map dimensions and the encoder structure to extract contextual data. Swin-UNet has outperformed previous Transformer techniques on a number of medical image segmentation tasks thanks to its U-shaped topology, which combines high-level and low-level data without the disadvantages of convolution.
Transformers’ parallelized training improves their ability to capture detailed data. This architecture, which is based only on attention techniques, can highlight important characteristics while suppressing unimportant background. In liver tumor segmentation jobs, this helps locate tumors quickly and reliably [
103].
A pure ViT encoder that operates on 3D medical volumes and is coupled to a CNN decoder by skip connections at several transformer output levels was suggested by UNETR [
22] as a complete replacement for the CNN encoder. UNETR captures global spatial interdependence from the very beginning of encoding by tokenizing the 3D volume into fixed-size cubic patches. Although its quadratic attention complexity restricted it to somewhat coarse patch sizes (16³ voxels), UNETR demonstrated competitive performance on the Medical Segmentation Decathlon liver task.
The Swin UNETR variation [
104] achieved state-of-theart performance on several organs, including the liver, by combining the effective Swin Transformer encoder with the UNETR decoder framework for 3D medical image segmentation. The effectiveness of self-supervised pre-training for transformer-based medical segmentation models was demonstrated by pre-training on large unlabeled CT datasets using masked volume inpainting (self-supervised pre-training), which significantly increased fine-tuning performance in labeled data regimes.
Transformer-based architectures entered the field of medical image segmentation in 2021 and have since achieved state-of-the-art performance on benchmarks for liver tumors by utilizing multi-head self-attention to capture long range spatial relationships.
Fig. 7 presents a comparative schematic analysis of three prominent DL architectures tailored for image segmentation tasks in medical imaging: the convolutional U-Net, the hybrid TransUNet, and the hierarchical, transformer-driven Swin UNETR. Transformer and foundation model approaches are compared in
Table 5 in terms of dimensionality, type, architecture, tumor DSC, and LiTS performance.
FOUNDATION MODELS AND PROMOTABLE SEGMENTATION
In 2023, Kirillov et al. [
24] at Meta AI introduced the SAM, which was a paradigm-shifting advancement in image segmentation. SAM showed remarkable zero-shot generalization to unseen segmentation tasks across various image domains whether prompted with points, bounding boxes, or text after being trained on an unprecedentedly huge dataset of over 1 billion masks obtained from 11 million genuine photos. However, SAM’s direct application to medical images a domain with statistical characteristics that are fundamentally different from those of nature photographs revealed notable performance gaps, with reported Dice scores on liver tumor segmentation tasks significantly lower than those of specialized supervised models.
Medical applications of SAM were quickly developed by several organizations. MedSAM [
105] significantly improved zero-shot and few-shot performance on unseen medical segmentation tasks by fine-tuning SAM on a sizable curated dataset of over a million medical image-mask pairings covering CT, MRI, PET, and ultrasound across numerous organs and modalities. Using slice-level bounding boxes and 3D point prompts for training, SAM-Med2D [
106] and SAMMed3D [
107] expanded medical SAM adaption to 3D volumetric segmentation. Flexible interaction modalities were made possible by SegVol’s [
108] integration of volumetric SAM with visual and semantic (text) cues. With the crucial benefit of requiring little to no task-specific training data, these medical SAM variants have shown competitive performance with supervised baselines on liver tumor benchmarks.
A new frontier where text-guided segmentation, clinical report creation, and multi-modal reasoning are combined is represented by the integration of large language models with medical image analysis, as demonstrated by models such as LLaVA-Med [
109] and MedPaLM-M [
110]. A revolutionary path for clinical integration is represented by the possibility of interactive, conversational segmentation systems that take natural language commands. However, there are still significant obstacles to overcome, including interpretability, robustness to adversarial prompts, safety validation in high-stakes clinical settings, and the computing demands of implementing billion-parameter foundation models at scale in clinical processes.
COMPARATIVE ANALYSIS AND DISCUSSION
A review of the literature covering the entire history of DL for liver tumor segmentation identifies a number of recurring patterns and important discoveries. From residual and attention-enhanced CNNs (DSC 0.65-0.81 on LiTS) to contemporary transformer and hybrid designs (DSC 0.70-0.85 on LiTS) and self-configuring frameworks like nnU-Net, the area has witnessed a monotonic improvement in performance. However, direct comparisons between articles are complicated by variations in evaluation procedures, cross-validation techniques, preprocessing, and the particular sample of LiTS cases assessed (training vs. test split), so absolute performance figs must be regarded with caution.
Second, only a small portion of performance improvements can be attributed to architectural innovation alone. Data preparation, augmentation technique, loss function design, and training protocol all make significant contributions, frequently more so than the particular network architecture. An excellent example of this idea is the success of nnU-Net, which uses comparatively ordinary 3D U-Net topologies but with highly streamlined data pipelines and training methodologies. Third, there are concerns about the practical usefulness of state-of-the-art techniques in clinical settings with limited resources due to their growing complexity and computational cost, especially transformer-based architectures. The marginal performance gains of highly complex models might not be sufficient to cover their computational overhead.
Fourth, there is still a significant and inadequately described discrepancy between performance on benchmark datasets and actual clinical performance. Benchmark datasets are crucial for repeatable comparison, but they don’t fully capture the diversity of clinical data due to selection bias, curation artifacts, and protocol standardization. There are still few multi-site prospective validation studies in the literature. Fifth, clinically significant aspects of segmentation quality, such as accuracy of lesion detection (differentiating true lesions from benign findings), boundary accuracy for particular applications (radiation therapy planning), and consistency across repeated measurements, are not fully captured by the evaluation metrics used in the majority of papers, especially DSC and HD95.
FUTURE DIRECTIONS
The advancement of liver tumor segmentation toward clinical utility is particularly promising in a number of research areas. The most revolutionary approach in the near future is the creation of fully universal medical image segmentation models that can perform few-shot or zero-shot generalization and are trained on vast amounts of varied imaging data spanning organs, modalities, and diseases. If trained on a large enough scale and thoroughly validated, models similar to medical SAM [
24], SegVol [
108], and Universal Model could significantly lessen the annotation effort for novel clinical tasks. The automated segmentation and quantitative comparison of tumor volumes over successive imaging time points, known as longitudinal tumor tracking, is still a clinically underutilized and technically difficult task. In order to increase segmentation consistency and enable biologically meaningful growth rate and treatment response analysis, current approaches treat each image independently, ignoring the chance to take advantage of temporal correlation. It is necessary to use temporal models with motion compensation, change detection, and deformable registration.
The detection of small and unclear lesions may be greatly enhanced by multi-modal fusion, which processes CT and MRI together or multi-phase CT to take advantage of complementary information. Each fusion strategy has unique benefits and drawbacks, ranging from early fusion (channel concatenation) to intermediate feature fusion to late fusion (ensemble of modality-specific predictions). A related approach is cross-modal synthesis to create missing modalities [
111]. A natural link between segmentation and clinical prediction tasks is provided by radiomics DL integration, which combines quantitative radiomic data collected from segmented tumor volumes with deep feature representations for prognostic modeling.
Given the strict patient data security rules (HIPAA, GDPR) in the medical field, federated learning [
112] and differentiated privacy techniques are crucial facilitators of multi-institutional collaboration without data sharing. Federated learning presents novel technological issues such as model aggregation under different local dataset sizes, heterogeneous data distributions across locations (statistical heterogeneity), and communication efficiency. A vibrant and quickly developing field of study is the creation of reliable federated learning techniques for medical image segmentation.
Lastly, safe and efficient clinical deployment depends on the creation of AI systems that complement rather than replace radiologists’ skills. Examples of these systems include human in the loop refinement, interactive segmentation with little user input, and uncertainty-guided review prioritizing. Active learning frameworks can minimize annotation costs and speed up the generation of better models by dynamically choosing the most informative cases for expert annotation. To offer the evidence base for broad clinical adoption, rigorous prospective clinical trials evaluating the effects of AI-assisted liver tumor segmentation on clinical workflow efficiency, inter-observer variability, and patient outcomes are desperately needed.
CONCLUSION
DL techniques for liver tumor segmentation in abdominal CT and MRI images have been thoroughly and methodically surveyed in this review, which traces the development of the field from the fundamental U-Net architecture through residual and attention-enhanced CNNs, transformer-based and hybrid architectures, and the new paradigm of foundation models and promptable segmentation. Over the past ten years, the discipline has advanced significantly, with cutting-edge techniques attaining Dice scores above 0.75–0.80 on the LiTS standard for tumor segmentation performance that approaches clinical relevance for numerous lesion types and therapeutic applications. The crucial role of 3D volumetric processing for capturing inter-slice spatial context; the consistent advantage of cascaded two-stage pipelines for managing class imbalance; the complementarity of CNN local feature extraction and transformer global context modeling in hybrid architectures; the crucial role of data augmentation, self-supervised pre-training, and loss function design alongside architectural innovation; and the significant remaining challenges of small lesion detection, domain adaptation, and prospective clinical validation are just a few of the review’s points. The creation of large-scale, diverse, and multi-modal annotated datasets; standardization of evaluation protocols that allow for meaningful cross-paper comparison; thorough multi-site prospective clinical validation studies; and responsible development of AI systems that are interpretable, uncertainty-aware, and intended for safe clinical integration are the field’s top priorities. AI-driven liver tumor segmentation has real potential to increase diagnostic precision, lessen workload, and eventually improve outcomes for liver cancer patients with further advancements in these areas.
NOTES
-
ACKNOWLEDGEMENTS
In this article, ChatGPT model 5.4 (OpenAI, CA, USA) was used for refining texts and drafting schematics and diagrams in Figures. All content was reviewed for accuracy and coherence.
-
FUND
This study was supported by the BK21 Four project funded by the Ministry of Education, Korea (4199990113966).
-
ETHICS STATEMENT
Not applicable.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Saif Ur Rehman Khan & Hyunyeol Lee: Conceptualization, Data curation, Methodology, Software, Validation, Writing original draft & Formal analysis.
SUPPLEMENTARY MATERIAL
The references cited in Tables 1–5 are provided in the Supplementary Materials.
Figure 1.AI pipeline for liver cancer diagnosis. CT, computed tomography; MRI, magnetic resonance imaging.

Figure 2.PRISMA flow diagram systematic review of DL for liver tumor segmentation. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; DL, deep learning.
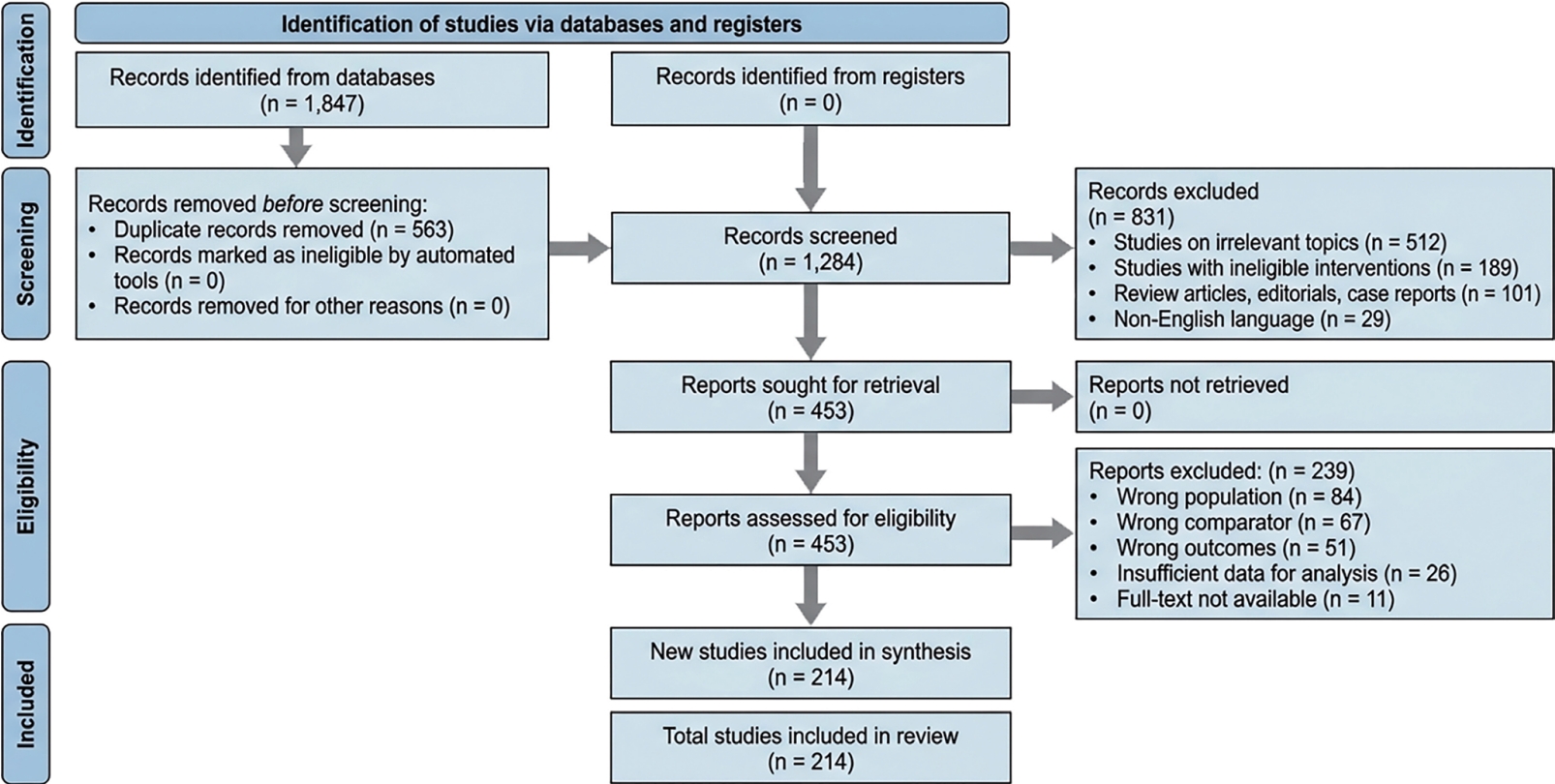
Figure 3.Overview of the primary imaging techniques for liver tumor analysis.
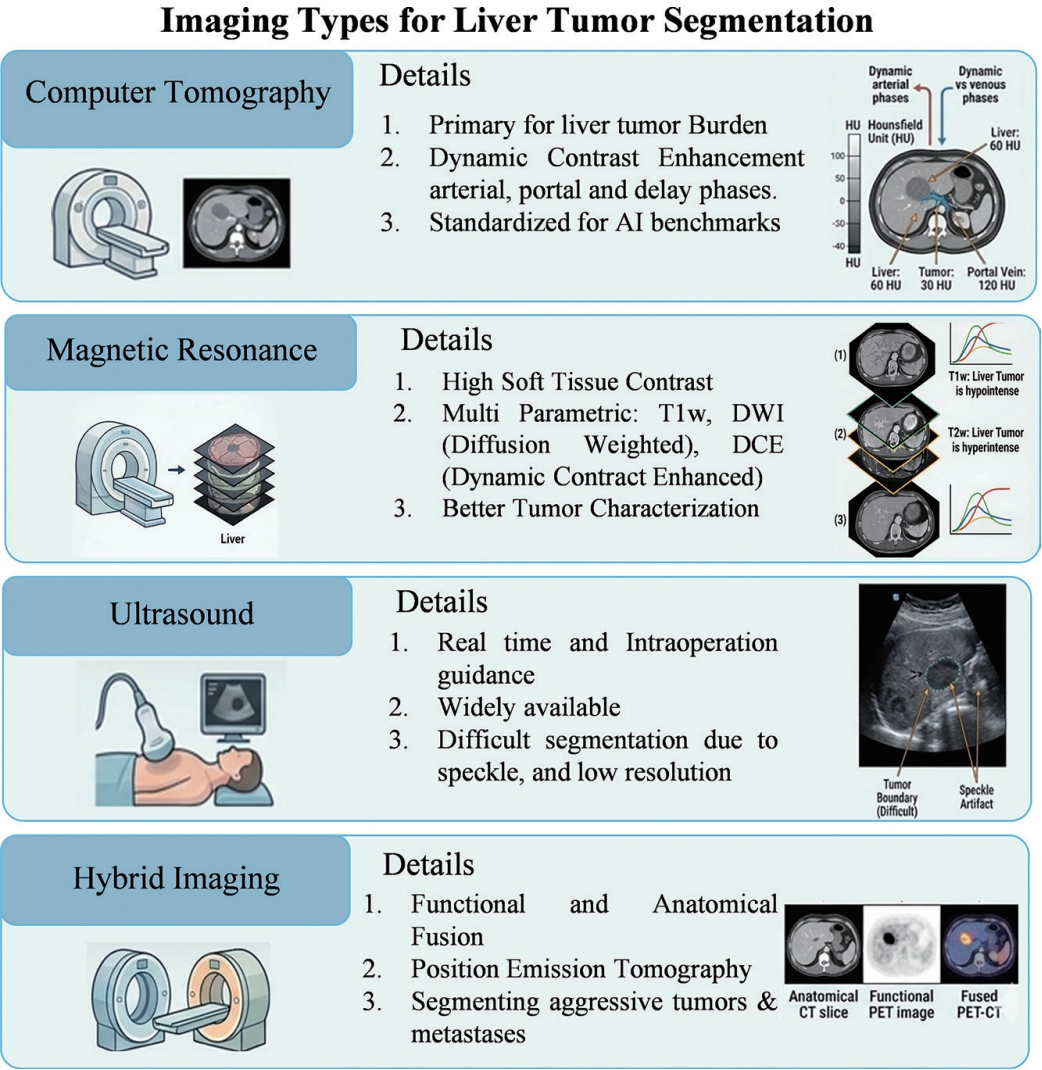
Figure 4.Overview of the primary methodologies used for liver tumor segmentation.
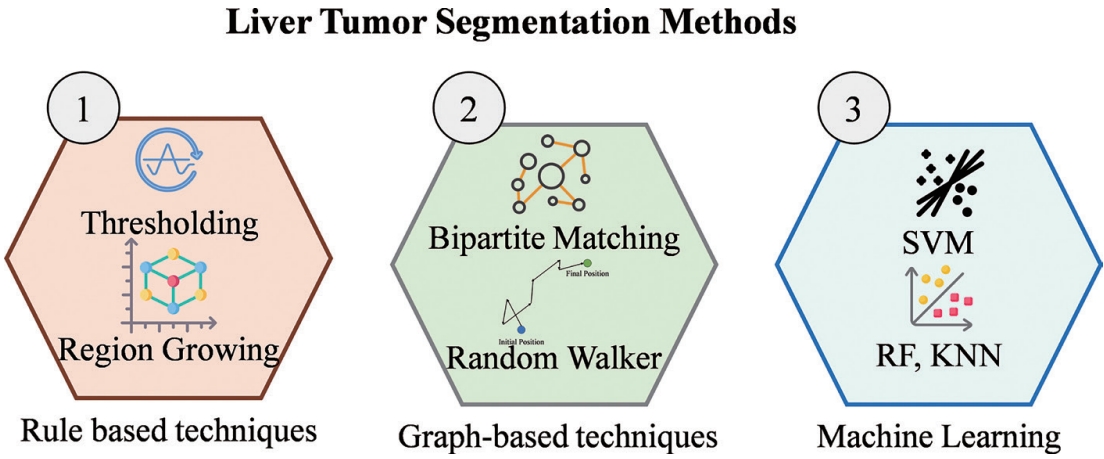
Figure 5.Architecture of evolution of medical image segmentation. CNN, convolutional neural networks; SAM, Segment Anything Model.
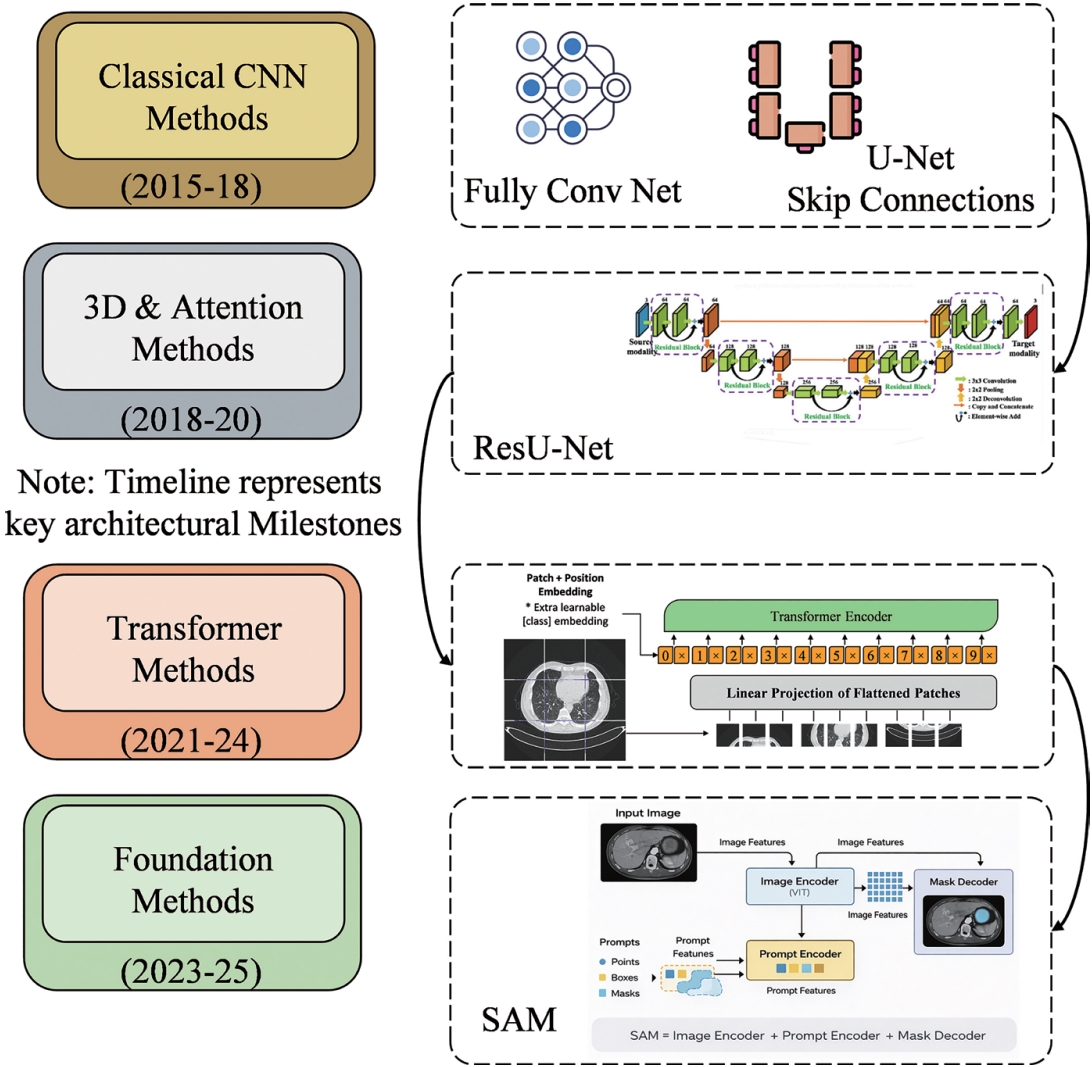
Figure 6.Architecture of CNN (A) and FCN (B). CNN, convolutional neural networks; FCN, Fully Convolutional Network.
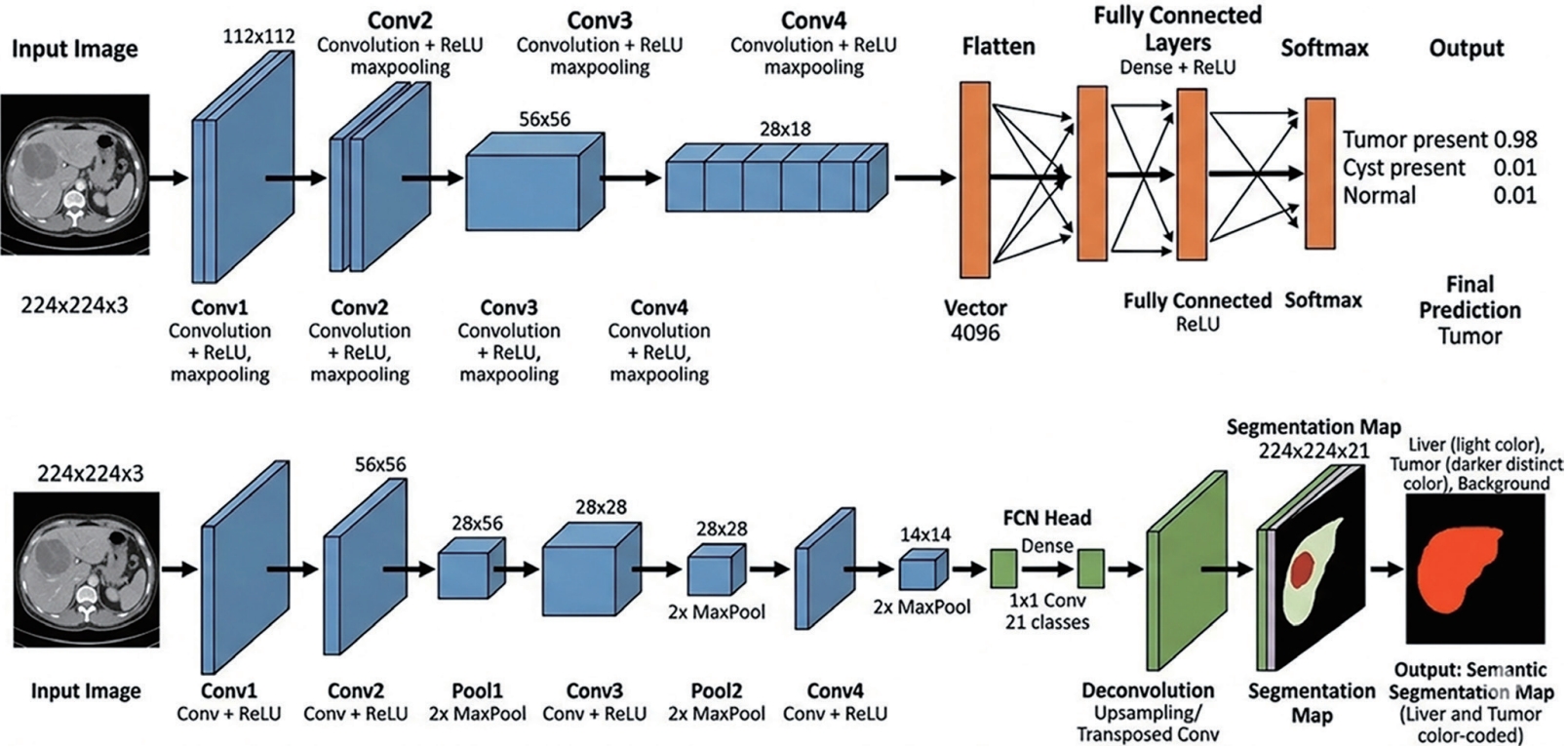
Figure 7.Comparative analysis of three representative DL architectures of image segmentation. Transformer based and Foundation Model Methods for Liver Tumor Segmentation. DL, deep learning; CNN, convolutional neural networks; CT, computed tomography; MRI, magnetic resonance imaging.
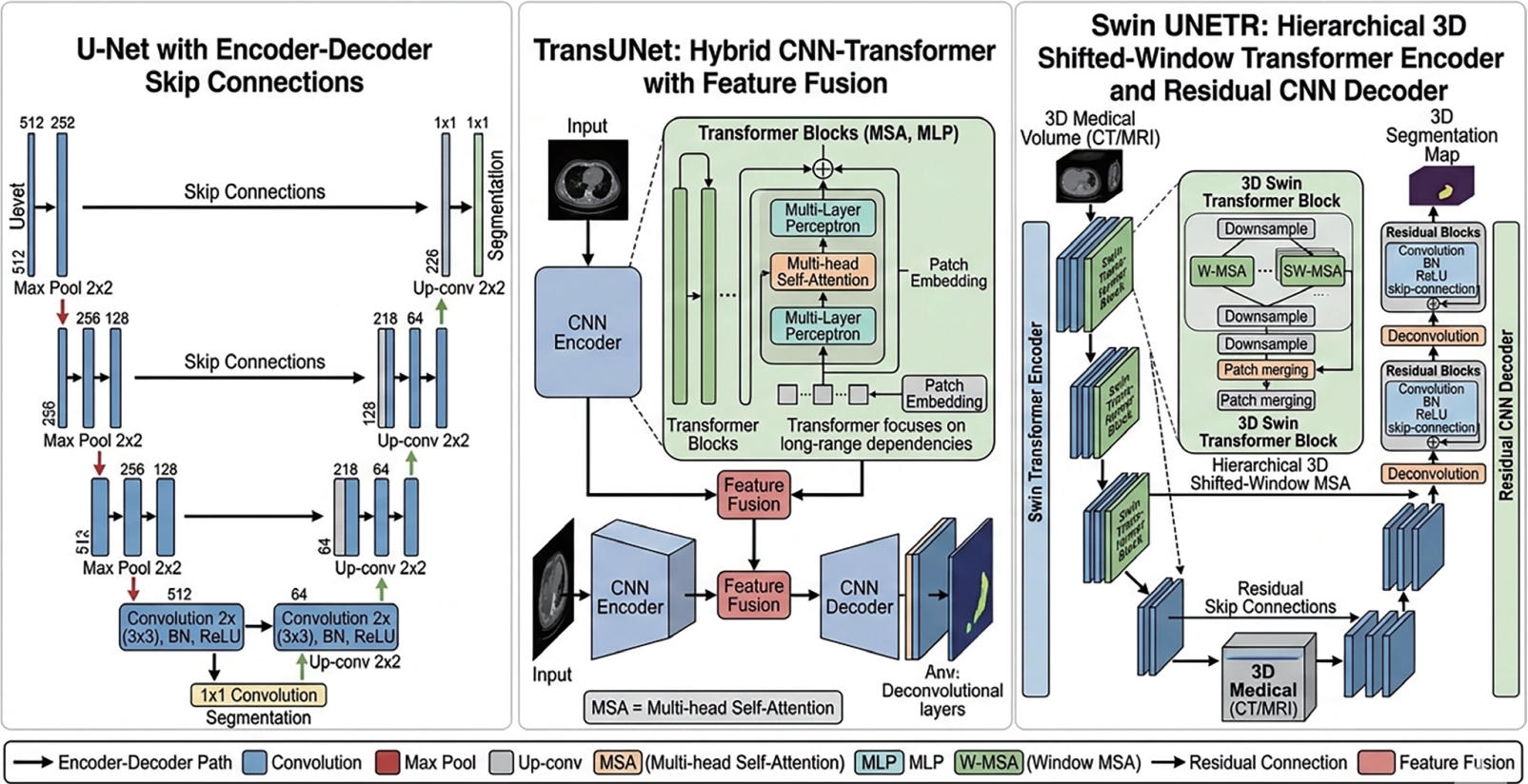
Table 1.Summary of key publicly available liver tumor segmentation datasets
Table 1.
|
Dataset |
Size |
Annotations |
Source |
|
LiTS (Bilic et al., 2023 [62]) |
201 |
Liver/tumor masks |
CT |
|
3D-IRCADb (Soler et al., 2010 [63]) |
20 |
Liver, tumors, vessels |
CT |
|
SLIVER07 (Heimann et al., 2009 [64]) |
30 |
Liver delineations |
CT |
|
CHAOS (Kavur et al., 2021 [65]) |
80 |
Healthy liver, kidneys, and spleen |
CT/MRI |
|
MSD (Antonelli et al., 2022) |
443 |
Liver, tumor, vessels |
CT |
|
ATLAS (Quinton et al., 2023 [66]) |
60 |
HCC, liver, tumors |
MRI |
|
TCGA-LIHC (Shi et al., 2025) |
75 |
Phenotypes, tumors |
CT/MRI/PET |
|
LiVS (Zhao 2022) |
532 |
Liver vessel annotations |
CT |
|
LiTS-PAIP 2019 (Kim et al., 2021) |
100 |
Liver cancer regions |
Histopathology |
|
AbdomenCT-1K (Ma et al., 2022 [56]) |
1112 |
Multiple organs |
CT |
|
TotalSegmentator (Wasserthal et al., 2023 [67]) |
1204 |
liver, tumors |
CT |
|
WORD (Luo et al., 2022) |
170 |
Abdominal organs |
CT |
|
BTCV (Landman et al., 2015) |
50 |
Abdominal organs |
CT |
|
VISCERAL (Jimenez-del-Toro et al., 2016) |
60 |
liver anatomy segmentation |
CT/MRI |
|
CLUST (De Luca et al., 2015) |
86 |
Liver tracking points |
Ultrasound |
|
DLDS (Macdonald et al., 2023) |
426 |
Liver masks |
MRI |
|
Barts CRL (Abdoli et al., 2025) |
220 |
Liver metastases |
CT |
|
NucleiSegNet (Lal et al., 2021) |
80 |
Semantic features |
Histopathology |
|
CLEF 2015 |
60 |
Structured reporting |
CT |
|
LTSC08 (Deng and Du 2008) |
30 |
Liver lesions/tumors |
CT |
|
AMOS22 (Bai et al., 2022) |
500/100 |
Multi organ masks |
CT and MRI |
|
VASCUSYNTH (Hamarneh and Jassi 2010) |
120 |
Synthetic vessels |
Synthetic CT |
Table 2.Evaluation metrics used in liver tumor segmentation benchmarks
Table 2.
|
Metric |
Formula |
Range |
Strength |
Limitation |
|
Dice (DSC) (Milletari et al., 2016 [15]) |
2|A∩B||A|+|B|
|
0–1 ↑ |
Overlap measure; most reported |
Sensitive to class size |
|
IoU/Jaccard (Everingham et al., 2010) |
|A∩B||A∪B|
|
0–1 ↑ |
Related to DSC; DSC/(2-DSC) |
Sensitive to class size |
|
Hausdorff (HD) (Huttenlocher et al., 2002) |
max surface distance |
mm ↓ |
Captures worst-case boundary error |
Sensitive to outliers |
|
HD95 |
95th percentile HD |
mm ↓ |
Robust boundary accuracy |
Needs full surface mesh |
|
Sensitivity (Fawcett 2006) |
TP/(TP+FN) |
0–1 ↑ |
Lesion detection rate |
Ignores specificity |
|
Precision (PPV) (Sokolova and Lapalme 2009) |
TP/(TP+FP) |
0–1 ↑ |
Low false positive rate |
Trade-off with sensitivity |
|
RVD (Heimann et al., 2009 [64]) |
|A|−|B||B|
|
% ↓ |
Volume difference |
No shape information |
|
Surface DSC (Nikolov et al., 2018) |
Fraction within τ mm |
0–1 ↑ |
Clinically interpretable boundary |
Threshold τ dependent |
|
Average Surface Distance (ASD) (Heimann et al., 2009 [64]) |
∑a∈SAda,SB+∑b∈Sbdb,SASA+SB
|
0–∞ ↓ |
Measures average boundary distance between segmentation and ground truth |
Sensitive to boundary errors |
|
Volumetric Overlap Error (VOE) (Crum et al., 2006) |
1−|A∩B||A∪B|
|
0–1 ↑ |
Measure of segmentation mismatch by directly quantifying overlap error between predicted and reference regions |
Sensitive to boundary inaccuracies |
Table 3.Pre-DL methods for liver tumor segmentation
Table 3.
|
Method |
Era |
Modality |
Key Mechanism |
Tumor DSC ↑ |
Liver DSC ↑ |
|
Region Growing (Adams and Bischof 1994) |
2000s |
CT/MRI |
Propagate from seed point by intensity+gradient criteria |
~0.45 |
~0.78 |
|
Active Contours (Snakes) (Kass et al., 1988 [37]) |
2001+ |
CT/MRI |
Energy minimisation evolving a contour toward boundaries |
~0.50 |
~0.80 |
|
Level-Set Methods (Osher and Sethian 1988 [38]) |
2004+ |
CT/MRI |
PDE-driven surface evolution; topologically flexible |
~0.52 |
~0.82 |
|
Graph Cut (Boykov and Jolly 2001 [39]) |
2006+ |
CT |
Min-cut energy minimisation on voxel graph |
~0.53 |
~0.83 |
|
Random Walker (Grady 2006) |
2006+ |
CT/MRI |
Probabilistic random walk from user-placed seeds |
~0.50 |
~0.81 |
|
Multi-Atlas + STAPLE (Warfield et al., 2004) |
2009+ |
CT |
Label fusion from multiple registered atlases |
~0.52 |
~0.87 |
|
SVM + Hand-Crafted Features (Cortes and Vapnik 1995) |
2010+ |
CT/MRI |
Classify voxels using Haar, Gabor, LBP, HOG features |
~0.55 |
~0.84 |
|
Random Forest (Cutler et al., 2012) |
2012+ |
CT |
Ensemble of decision trees on handcrafted features |
~0.57 |
~0.86 |
|
Markov Random Field (MRF) (Li et al., 2005 [42]) |
2008+ |
CT |
Bayesian spatial regularisation of voxel labels |
~0.53 |
~0.83 |
|
Conditional Random Field (CRF) (Lafferty et al., 2001) |
2011+ |
CT/MRI |
Unary+pairwise energy on dense voxel graph |
~0.56 |
~0.85 |
|
Watershed + Morphology (Vincent and Soille 1991) |
2005+ |
CT |
Gradient-based flooding from markers+morphological ops |
~0.44 |
~0.78 |
|
Fuzzy C-Means Clustering (Bezdek et al., 1984) |
2005+ |
CT/MRI |
Unsupervised fuzzy partition of intensity space |
~0.42 |
~0.76 |
|
Coupled Level-Sets (Christ et al., 2017 [91]) |
2010+ |
CT |
Joint liver+tumour level-set evolution |
~0.54 |
~0.84 |
Table 4.CNN-based DL methods for liver tumor segmentation
Table 4.
|
Method |
Year |
Dim |
Type |
Architecture/Key feature |
Tumor DSC ↑ |
LiTS DSC ↑ |
|
U-Net (Ronneberger et al., 2015 [14]) |
2015 |
2D |
CE+Aug |
Enc-dec + concatenative skip connections |
~0.61 |
~0.65 |
|
3D U-Net (Çiçek et al., 2016 [95]) |
2016 |
3D |
CE |
Full 3D convolutions sparse annotation learning |
~0.68 |
~0.70 |
|
V-Net (Milletari et al., 2016 [15]) |
2016 |
3D |
Dice |
Residual 3D blocks + Dice loss; volumetric input |
~0.68 |
~0.72 |
|
ResU-Net (He et al., 2016 [16]) |
2017 |
2D/3D |
Dice |
Residual blocks in enc-dec pretrained backbone |
~0.70 |
~0.73 |
|
DenseU-Net (Huang et al., 2017 [97]) |
2017 |
2D |
Dice |
Dense connectivity within enc-dec blocks |
~0.71 |
~0.74 |
|
H-DenseUNet (Li et al., 2018 [96]) |
2018 |
2D+3D |
Dice |
Hybrid 2D slice + 3D volume dense connections |
~0.72 |
~0.76 |
|
UNet++ (Zhou et al., 2018 [93]) |
2018 |
2D |
Dice+CE |
Nested dense skip connections; deep supervision |
~0.73 |
~0.75 |
|
Attn U-Net (Oktay et al., 2018 [17]) |
2018 |
2D |
Focal |
Attention gates on skip connections from decoder |
~0.72 |
~0.74 |
|
SE-UNet (Hu et al., 2018 [99]) |
2018 |
2D/3D |
Dice |
Channel-wise squeeze-excitation recalibration |
~0.73 |
~0.75 |
|
CBAM-UNet (Woo et al., 2018 [100]) |
2018 |
2D |
Dice |
Channel + spatial attention in every conv block |
~0.73 |
~0.75 |
|
MS-UNet (Kushnure and Talbar 2021) |
2021 |
2D |
Dice+Focal |
Multi-scale feature recalibration across resolutions |
~0.74 |
~0.77 |
|
nnU-Net (Isensee et al., 2019) |
2021 |
2D/3D |
Dice+CE |
Self-configuring: auto preprocessing, patch, arch |
~0.75 |
~0.81 |
|
Cascade CNN (Christ et al., 2017 [91]) |
2017+ |
2D/3D |
Dice |
Stage1: liver crop → Stage2: tumour segment |
~0.78 |
~0.80 |
|
DeepMedic (Kamnitsas et al., 2017) |
2017 |
3D |
CE |
Multi-scale parallel 3D CNN paths |
~0.70 |
~0.72 |
Table 5.Transformer-based and foundation model methods for liver tumor segmentation
Table 5.
|
Method |
Year |
Dim |
Type |
Architecture/Key feature |
Tumor DSC ↑ |
LiTS DSC ↑ |
|
TransUNet (Chen et al., 2014 [20]) |
2014 |
2D |
Hybrid |
ResNet-50 encoder+ViT bottleneck + CNN decoder |
~0.81 |
~0.77 |
|
Swin-UNet (Cao et al., 2023 [21]) |
2023 |
2D |
Pure Trans. |
Pure Swin Transformer enc-dec with patch merging |
~0.81 |
~0.79 |
|
UNETR (Hatamizadeh et al., 2022 [22]) |
2022 |
3D |
Hybrid |
ViT encoder (16³ patches)+CNN residual decoder |
~0.82 |
~0.80 |
|
nnFormer (Zhou et al., 2023 [23]) |
2022 |
3D |
Pure Trans. |
Interleaved local+global 3D self-attention blocks |
~0.83 |
~0.82 |
|
Swin UNETR (Hatamizadeh et al., 2022 [104]) |
2022 |
3D |
Hybrid |
Swin-T 3D encoder+residual CNN decoder + SSL |
~0.84 |
~0.83 |
|
HiFormer (Heidari et al., 2023) |
2022 |
2D |
Hybrid |
CNN+Swin at two scales; double-level fusion |
~0.80 |
~0.77 |
|
CvT-UNet (Wu et al., 2022) |
2022 |
2D |
Hybrid |
Convolutional projections in self-attention |
~0.80 |
~0.76 |
|
DS-TransUNet (Lin et al., 2022) |
2022 |
2D |
Hybrid |
Dual-scale Swin+CNN path with attention fusion |
~0.82 |
~0.79 |
|
MedT (Valanarasu et al., 2021) |
2021 |
2D |
Pure Trans. |
Gated axial attention+local-global training |
~0.79 |
~0.75 |
|
SegFormer (Xie et al., 2021) |
2022 |
2D |
Hybrid |
Mix-Transformer encoder+lightweight MLP decoder |
~0.80 |
~0.77 |
|
UNETR++ (Shaker et al., 2024) |
2023 |
3D |
Hybrid |
Efficient paired attention; reduce UNETR compute |
~0.84 |
~0.82 |
|
SwinMM (Wang et al., 2023) |
2023 |
3D |
Hybrid |
Multi-view Swin+masked modelling pre-training |
~0.84 |
~0.82 |
|
SAM (Kirillov et al., 2023 [24]) |
2023 |
2D |
Foundation |
ViT-H encoder+prompt encoder + mask decoder |
~0.72 |
~0.70 |
|
MedSAM (Ma et al., 2024 [105]) |
2024 |
2D/3D |
Foundation |
SAM fine-tuned on 1.5M medical image-mask pairs |
~0.86 |
~0.85 |
|
SAM-Med3D (Wang et al., 2024 [107]) |
2024 |
3D |
Foundation |
3D SAM with volumetric point+box prompts |
~0.84 |
~0.82 |
REFERENCES
- 1. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol 2022;77:1598-1606.
- 2. Chou R, Cuevas C, Fu R, et al. Imaging techniques for the diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Ann Intern Med 2015;162:697-711.
- 3. Fass L. Imaging and cancer: a review. Mol Oncol 2008;2:115-152.
- 4. Yeh BM, FitzGerald PF, Edic PM, et al. Opportunities for new CT contrast agents to maximize the diagnostic potential of emerging spectral CT technologies. Adv Drug Deliv Rev 2017;113:201-222.
- 5. Schwartz LH, Litière S, de Vries E, et al. RECIST 1.1–update and clarification: from the RECIST committee. Eur J Cancer 2016;62:132-137.
- 6. Radtke A, Nadalin S, Sotiropoulos GC, et al. Computer-Assisted operative planning in adult living donor liver transplantation: a new way to resolve the dilemma of the middle hepatic vein. World J Surg 2007;31:175-185.
- 7. Zhou YJ, Tang Y, Liu SJ, et al. Radiation-induced liver disease: Beyond DNA damage. Cell Cycle 2023;22:506-526.
- 8. Shehta A, Elsabbagh AM, Medhat M, et al. Impact of tumor size on the outcomes of hepatic resection for hepatocellular carcinoma: A retrospective study. BMC Surg 2024;24:7.
- 9. Chen Z, Zheng H, Zeng W, Liu M, Chen Y. Prognostic analysis on different tumor sizes for 14634 hepatocellular carcinoma patients. Eur J Cancer Care (Engl) 2023;2023:1106975.
- 10. Baâzaoui A, Barhoumi W, Ahmed A, Zagrouba E. Semi-automated segmentation of single and multiple tumors in liver CT images using entropy-based fuzzy region growing. IRBM 2017;38:98-108.
- 11. Zhang Y, Yang J, Liu Y, et al. Decoupled pyramid correlation network for liver tumor segmentation from CT images. Med Phys 2022;49:7207-7221.
- 12. Li JF, Niu YM. Dual encoding DDS-UNet liver tumour segmentation based on multi-scale deep and shallow feature fusion. IET Image Process 2024;18:1189-1199.
- 13. Ansari MY, Abdalla A, Ansari MY, et al. Practical utility of liver segmentation methods in clinical surgeries and interventions. BMC Med Imaging 2022;22:97.
- 14. Ronneberger O, Fischer P, Brox T. U-Net: convolutional networks for biomedical image segmentation. In Navab N, Hornegger J, Wells WM, Frangi AF, editors. Medical Image Computing and Computer-Assisted Intervention – MICCAI 2015. Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2015. p.234-241.
- 15. Milletari F, Navab N, Ahmadi SA. V-Net: fully convolutional neural networks for volumetric medical image segmentation. In: Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV). Stanford (CA), USA: IEEE; 2016. p.565-571.
- 16. He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Las Vegas (NV), USA: IEEE; 2016. p.770-778.
- 17. Oktay O, Schlemper J, Le Folgoc L, et al. Attention U-Net: learning where to look for the pancreas. arXiv 1804.03999 [Preprint]. 2018. doi: 10.48550/arXiv.1804.03999.
- 18. Huang G, Liu Z, Pleiss G, Maaten LV, Weinberger KQ. Convolutional networks with dense connectivity. IEEE Trans Pattern Anal Mach Intell 2022;44:8704-8716.
- 19. Dosovitskiy A, Beyer L, Kolesnikov A, et al. An image is worth 16x16 words: transformers for image recognition at scale. arXiv 2010.11929 [Preprint]. 2020. doi: 10.48550/arXiv.2010.11929.
- 20. Chen J, Lu Y, Yu Q. Transunet: Transformers make strong encoders for medical image segmentation. arXiv 2102.04306 [Preprint]. 2014. doi: 10.48550/arXiv.2102.04306.
- 21. Cao H, Wang Y, Chen J, et al. Swin-Unet: U-Net-like pure transformer for medical image segmentation. In Karlinsky L, Michaeli T, Nishino K, editors. Computer Vision – ECCV 2022 Workshops. Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2023. p.205-218.
- 22. Hatamizadeh A, Tang Y, Nath V, Yang D, Roth HR, Xu D. UNETR: transformers for 3D medical image segmentation. In: Proceedings of the IEEE/CVF Winter Conference on Applications of Computer Vision (WACV). Waikoloa (HI), USA: IEEE; 2022. p.574-584.
- 23. Zhou HY, Guo J, Zhang Y, et al. Nnformer: Volumetric medical image segmentation via a 3d transformer. IEEE Trans Image Process 2023;32:4036-4045.
- 24. Kirillov A, Mintun E, Ravi N, et al. Segment Anything. In: Proceedings of the IEEE/CVF International Conference on Computer Vision (ICCV). Paris (France): IEEE; 2023. p.4015-4026.
- 25. Saha A, van der Pol CB. Liver observation segmentation on contrast-enhanced MRI: SAM and MedSAM performance in patients with probable or definite hepatocellular carcinoma. Can Assoc Radiol J 2024;75:771-779.
- 26. Zeng L, Liu Z, Wang X, Wu Z, Ju X, Zhu YC, Zhang C. Context-aware multi-organ segmentation in abdominal CT via LoRA-fine-tuned Med-SAM. In: 2024 IEEE International Conference on Bioinformatics and Biomedicine (BIBM). IEEE; 2024. p.3966-3971.
- 27. Vrabel M. Preferred reporting items for systematic reviews and meta-analyses. Oncol Nurs Forum 2015;42:552-554.
- 28. Ma J, Li F, Wang B. U-Mamba: enhancing long-range dependency for biomedical image segmentation. arXiv 2401.04722 [Preprint]. 2024. doi: 10.48550/arXiv.2401.04722.
- 29. Cao G, Yan R, Zhang Y, et al. Long-range sequential modeling Mamba for 3D abdominal multi-organ segmentation. In: 2024 9th International Conference on Intelligent Informatics and Biomedical Sciences (ICIIBMS). IEEE; 2024. p.431-436.
- 30. Ruan J, Li J, Xiang S. VM-UNet: Vision Mamba UNet for medical image segmentation. ACM Trans Multimedia Comput Commun Appl 2024;doi: 10.1145/3767748.
- 31. Zhu J, Hamdi A, Qi Y, Jin Y, Wu J. Medical SAM 2: segment medical images as video via Segment Anything Model 2. arXiv 2408.00874 [Preprint]. 2024. doi: 10.48550/arXiv.2408.00874.
- 32. Dong H, Gu H, Chen Y, Yang J, Chen Y, Mazurowski MA. Segment anything model 2: an application to 2D and 3D medical images. IEEE Trans Biomed Eng 2026 Jan 12. doi:10.1109/TBME.2026.3653267.
- 33. Wu J, Fu R, Fang H, et al. MedSegDiff: medical image segmentation with diffusion probabilistic model. In: Proceedings of the 6th Medical Imaging with Deep Learning Conference (MIDL). Proceedings of Machine Learning Research 2024;227:1623-1639.
- 34. Wu J, Ji W, Fu H, Xu M, Jin Y, Xu Y. Medsegdiff-v2: Diffusion-based medical image segmentation with transformer. AAAI 2024;38:6030-6038.
- 35. Delmoral JC, Tavares JMR. Semantic segmentation of CT liver structures: a systematic review of recent trends and bibliometric analysis: Neural network-based methods for liver semantic segmentation. J Med Syst 2024;48:97.
- 36. Sethia K, Strakos P, Jaros M, et al. Advances in liver, liver lesion, hepatic vasculature, and biliary segmentation: a comprehensive review of traditional and deep learning approaches. Artif Intell Rev 2025;58:299.
- 37. Kass M, Witkin A, Terzopoulos D. Snakes: Active contour models. Int J Comput Vision 1988;1:321-331.
- 38. Osher S, Sethian JA. Fronts propagating with curvature-dependent speed: algorithms based on Hamilton-Jacobi formulations. J Comput Phys 1988;79:12-49.
- 39. Boykov YY, Jolly M. Interactive graph cuts for optimal boundary & region segmentation of objects in ND images. Proc Eighth IEEE Int Conf Comput Vis ICCV 2001 None;1:105-112.
- 40. Ugo L, Brocco S, Merola A, Mescoli C, Quaia E. Liver anatomy. In: Quaia E, editor. Imaging of the liver and intra-hepatic biliary tract. Vol 1: imaging techniques and non-tumoral pathologies. Cham (Switzerland): Springer; 2021. p.11-34.
- 41. Withers PJ, Bouman CA, Carmignato S, et al. X-ray computed tomography. Nat Rev Methods Primers 2021;1:18.
- 42. Li C, Xu C, Gui C, Fox MD. Level set evolution without re-initialization: a new variational formulation. In: Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR). San Diego (CA), USA: IEEE; 2005. p.430-436.
- 43. Cheng CT, Ooyang CH, Liao CH, Kang SC. Applications of deep learning in trauma radiology: a narrative review. Biomed J 2025;48:100743.
- 44. Wang R, Shi X, Pang S, et al. Cross-attention guided loss-based deep dual-branch fusion network for liver tumor classification. Inf 2025;114:102713.
- 45. Sun Y, Cheng Z, Qiu J, Lu W. Performance and application of the Total-Body PET/CT scanner: a literature review. EJNMMI Res 2024;14:38.
- 46. Meng K, Gong G, Liu R, Du S, Yin Y. Advances in Gross Tumor Target Volume Determination in Radiotherapy for Patients with Hepatocellular Carcinoma. Front Oncol 2024;14:1346407.
- 47. Liu Z, Song Y, Sheng VS, et al. Liver CT sequence segmentation based with improved u-Net and graph cut. Expert Syst Appl 2019;126:54-63.
- 48. Xia Z, Liao M, Di S, Zhao Y, Liang W, Xiong NN. Automatic liver segmentation from CT volumes based on multi-view information fusion and condition random fields. Opt Technol 2024;179:111298.
- 49. Huang S, Luo J, Ou Y, et al. Sd-Net: a semi-supervised double-cooperative network for liver segmentation from computed tomography (CT) images. J Cancer Res Clin Oncol 2024;150:79.
- 50. Zhu J, Liu Z, Gao W, Fu Y. CotepRes-Net: An efficient u-Net based deep learning method of liver segmentation from computed tomography images. Biomed Signal Process Control 2024;88:105660.
- 51. Ouyang S, He B, Luo H, Jia F. SwinD-Net: A lightweight segmentation network for laparoscopic liver segmentation. Comput Assist Surg (Abingdon) 2024;29:2329675.
- 52. Seo H, Huang C, Bassenne M, Xiao R, Xing L. Modified u-Net (mUNet) with incorporation of object-dependent high-level features for improved liver and liver-tumor segmentation in CT images. IEEE Trans Med Imaging 2020;39:1316-1325.
- 53. Xie X, Zhang W, Wang H, et al. Dynamic adaptive residual network for liver CT image segmentation. Comput Electr Eng 2021;91:107024.
- 54. Goryawala M, Gulec S, Bhatt R, McGoron AJ, Adjouadi M. A low-interaction automatic 3D liver segmentation method using computed tomography for selective internal radiation therapy. Biomed Res Int 2014;2014:198015.
- 55. Ou J, Jiang L, Bai T, Zhan P, Liu R, Xiao H. ResTransUnet: An effective network combined with Transformer and u-Net for liver segmentation in CT scans. Comput Biol Med 2024;177:108625.
- 56. Ma J, Zhang Y, Gu S, et al. Abdomenct-1k: Is abdominal organ segmentation a solved problem? IEEE Trans Pattern Anal Mach Intell 2022;44:6695-6714.
- 57. Lou Q, Lin T, Qian Y, Lu F. Semi-supervised liver segmentation based on local regions self-supervision. Med Phys 2024;51:3455-3463.
- 58. Lian Z, Lu Q, Lin B, et al. A fully automatic parenchyma extraction method for MRI T2* relaxometry of iron loaded liver in transfusion-dependent patients. Magn Reson Imaging 2024;109:18-26.
- 59. Okada T, Linguraru MG, Hori M, Summers RM, Tomiyama N, Sato Y. Abdominal multi-organ segmentation from CT images using conditional shape–location and unsupervised intensity priors. Med Image Anal 2015;26:1-18.
- 60. Peng J, Hu P, Lu F, Peng Z, Kong D, Zhang H. 3D liver segmentation using multiple region appearances and graph cuts. Med Phys 2015;42:6840-6852.
- 61. Ozkan S, Selver MA, Baydar B, Kavur AE, Candemir C, Akar GB. Cross-Modal learning via adversarial loss and covariate shift for enhanced liver segmentation. IEEE Trans Emerg Top Comput Intell 2024;8:2723-2735.
- 62. Bilic P, Christ P, Li HB, et al. The liver tumor segmentation benchmark (Lits). Med Image Anal 2023;84:102680.
- 63. Soler L, Hostettler A, Agnus V, et al. 3D image reconstruction for comparison of algorithm database: a patient specific anatomical and medical image database. Strasbourg (France). IRCAD. 2010, Technical report.
- 64. Heimann T, van Ginneken B, Styner MA, et al. Comparison and evaluation of methods for liver segmentation from CT datasets. IEEE Trans Med Imaging 2009;28:1251-1265.
- 65. Kavur AE, Gezer NS, Barış M, et al. CHAOS challenge-combined (CT-MR) healthy abdominal organ segmentation. Med Image Anal 2021;69:101950.
- 66. Quinton F, Popoff R, Presles B, et al. A tumour and liver automatic segmentation (Atlas) dataset on contrast-enhanced magnetic resonance imaging for hepatocellular carcinoma. Data (Basel) 2023;8:79.
- 67. Wasserthal J, Breit HC, Meyer MT, et al. Totalsegmentator: robust segmentation of 104 anatomic structures in CT images. Radiol Artif Intell 2023;5:e230024.
- 68. Luessi M, Eichmann M, Schuster GM, Katsaggelos AK. New results on efficient optimal multilevel image thresholding. In: Proceedings of the IEEE International Conference on Image Processing (ICIP). Atlanta (GA), USA: IEEE; 2006. p.773-776.
- 69. Lu X, Wu J, Ren X, Zhang B, Li Y. The study and application of the improved region growing algorithm for liver segmentation. Optik (Stuttg) 2014;125:2142-2147.
- 70. Pratondo A, Ong SH, Chui CK. Region growing for medical image segmentation using a modified multiple-seed approach on a multi-core CPU computer. In: Proceedings of the 15th International Conference on Biomedical Engineering (IFMBE Proceedings). Singapore: Springer; 2014. p.112-115.
- 71. Lohare DN, Manza RR, Tiwari N. Comparative study of Prewitt and Canny edge detector using image processing techniques. In Rathore VS, Dey N, Piuri V, Babo R, Polkowski Z, Tavares JMR, editors. Rising threats in expert applications and solutions: proceedings of FICR-TEAS 2020. Singapore: Springer; 2021. p.705-714.
- 72. Zenian S, Ahmad T, Idris A. Edge detection of flat electroencephalography image via classical and fuzzy approach. In Berry MW, Mohamed AH, Yap BW, editors. Soft Computing in Data Science: Second International Conference (SCDS 2016). Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2016. p.247-255.
- 73. Hervella ÁS, Rouco J, Novo J, Ortega M. Multimodal image encoding pre-training for diabetic retinopathy grading. Comput Biol Med 2022;143:105302.
- 74. Hariharan S, Anandan D, Krishnamoorthy M, Kukreja V, Goyal N, Chen S. Advancements in liver tumor detection: a comprehensive review of various deep learning models. CMES 2025;142:91-122.
- 75. Li BN, Chui CK, Chang S, Ong SH. A new unified level set method for semi-automatic liver tumor segmentation on contrast-enhanced CT images. Expert Syst Appl 2012;39:9661-9668.
- 76. Rahman F, Das D, Sami A, Podder P, Michael DL. Liver cirrhosis prediction using logistic regression, naı̈ve bayes and KNN. Int J Sci Res Arch 2024;12:2411-2420.
- 77. Guo B, Guo Y, Nima Q, et al. Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease. J Hepatol 2022;76:518-525.
- 78. Nigatu SS, Alla PCR, Ravikumar RN, Mishra K, Komala G, Chami GR. A comparative study on liver disease prediction using supervised learning algorithms with hyperparameter tuning. In: 2023 International Conference on Advancement in Computation and Computer Technologies (InCACCT). IEEE; 2023. p.353-357.
- 79. Li TS, Chiu H, Kuo P. Hepatitis c virus detection model by using random forest, logistic-regression and ABC algorithm. IEEE 2022;10:91045-91058.
- 80. Alizargar A, Chang YL, Alkhaleefah M, Tan TH. Precision non-alcoholic fatty liver disease (NAFLD) diagnosis: leveraging ensemble machine learning and gender insights for cost-effective detection. Bioengineering (Basel) 2024;11:600.
- 81. Zhao J, Wang P, Pan Y. Predicting liver disorder based on machine learning models. J Eng 2022;2022:978-984.
- 82. Malik S, Tenorio BG, Moond V, Dahiya DS, Vora R, Dbouk N. Systematic review of machine learning models in predicting the risk of bleed/grade of esophageal varices in patients with liver cirrhosis: a comprehensive methodological analysis. J Gastroenterol Hepatol 2024;39:2043-2059.
- 83. Huang SY, Hsu WL, Hsu RJ, Liu DW. Fully convolutional network for the semantic segmentation of medical images: A survey. Diagnostics (Basel) 2022;12:2765.
- 84. Beaufrère A, Ouzir N, Zafar PE, et al. Primary liver cancer classification from routine tumour biopsy using weakly supervised deep learning. JHEP Rep 2024;6:101008.
- 85. Niño SB, Bernardino J, Domingues I. Algorithms for liver segmentation in computed tomography scans: a historical perspective. Sensors (Basel) 2024;24:1752.
- 86. Manjunath RV, Ghanshala A, Kwadiki K. Deep learning algorithm performance evaluation in detection and classification of liver disease using CT images. Multimed Tools Appl 2024;83:2773-2790.
- 87. Nilashi M, Ahmadi H, Shahmoradi L, Ibrahim O, Akbari E. A predictive method for hepatitis disease diagnosis using ensembles of neuro-fuzzy technique. J Infect Public Health 2019;12:13-20.
- 88. Lu MY, Chuang WL, Yu ML. The role of artificial intelligence in the management of liver diseases. Kaohsiung J Med Sci 2024;40:962-971.
- 89. Szegedy C, Liu W, Jia Y, et al. Going deeper with convolutions. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Boston (MA), USA: IEEE; 2015. p.1-9.
- 90. Long J, Shelhamer E, Darrell T. Fully convolutional networks for semantic segmentation. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Boston (MA), USA: IEEE; 2015. p.3431-3440.
- 91. Christ PF, Ettlinger F, Grün F, et al. Automatic liver and tumor segmentation of CT and MRI volumes using cascaded fully convolutional neural networks. arXiv 1702.05970 [Preprint]. 2017. doi: 10.48550/arXiv.1702.05970.
- 92. Sun C, Guo S, Zhang H, et al. Automatic segmentation of liver tumors from multiphase contrast-enhanced CT images based on FCNs. Artif Intell Med 2017;83:58-66.
- 93. Zhou Z, Siddiquee MMR, Tajbakhsh N, Liang J. Unet++: A nested u-Net architecture for medical image segmentation. Deep Learn Med Image Anal Multimodal Learn Clin Decis Support (2018) 2018;11045:3-11.
- 94. Huang H, Lin L, Tong R, et al. UNet 3+: a full-scale connected UNet for medical image segmentation. In: 2020 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP). Barcelona (Spain): IEEE; 2020. p.1055-1059.
- 95. Çiçek Ö, Abdulkadir A, Lienkamp SS, Brox T, Ronneberger O. 3D U-Net: learning dense volumetric segmentation from sparse annotation. In Ourselin S, Joskowicz L, Sabuncu MR, Unal G, Wells W, editors. Medical Image Computing and Computer-Assisted Intervention – MICCAI 2016. Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2016. p.424-432.
- 96. Li X, Chen H, Qi X, Dou Q, Fu CW, Heng PA. H-DenseUNet: Hybrid densely connected UNet for liver and tumor segmentation from CT volumes. IEEE Trans Med Imaging 2018;37:2663-2674.
- 97. Huang G, Liu Z, van der Maaten L, Weinberger KQ. Densely connected convolutional networks. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Honolulu (HI), USA: IEEE; 2017. p.4700-4708.
- 98. Bahdanau D, Cho K, Bengio Y. Neural machine translation by jointly learning to align and translate. arXiv 1409.0473 [Preprint]. 2014. doi: 10.48550/arXiv.1409.0473.
- 99. Hu J, Shen L, Sun G. Squeeze-and-excitation networks. In: Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR). Salt Lake City (UT), USA: IEEE; 2018. p.7132-7141.
- 100. Woo S, Park J, Lee J-Y, Kweon IS. CBAM: convolutional block attention module. In Ferrari V, Hebert M, Sminchisescu C, Weiss Y, editors. Proceedings of the European Conference on Computer Vision (ECCV 2018). Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2018. p.3-19.
- 101. Vaswani A, Shazeer N, Parmar N, et al. Attention is all you need. In: Advances in Neural Information Processing Systems 30 (NeurIPS 2017). Red Hook (NY): Curran Associates; 2017. p.5998-6008.
- 102. Wang W, Chen C, Ding M, Yu H, Zha S, Li J. TransBTS: multimodal brain tumor segmentation using transformer. In: de Bruijne M, et al, editor. Medical Image Computing and Computer-Assisted Intervention – MICCAI 2021. Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2021. p.109-119.
- 103. Li L, Ma H. Rdctrans u-Net: a hybrid variable architecture for liver Ct image segmentation. Sensors (Basel) 2022;22:2452.
- 104. Hatamizadeh A, Nath V, Tang Y, Yang D, Roth HR, Xu D. Swin UNETR: Swin transformers for semantic segmentation of brain tumors in MRI images. In: BrainLes 2021: Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries. Lecture Notes in Computer Science. Cham (Switzerland): Springer; 2022. p.272-284.
- 105. Ma J, He Y, Li F, Han L, You C, Wang B. Segment anything in medical images. Nat Commun 2024;15:654.
- 106. Cheng J, Ye J, Deng Z, et al. SAM-Med2D. arXiv 2308.16184 [Preprint]. 2023. doi: 10.48550/arXiv.2308.16184.
- 107. Wang H, Guo S, Ye J, et al. SAM-Med3D: towards general-purpose segmentation models for volumetric medical images. arXiv 2310.15161 [Preprint]. 2023. doi: 10.1109/TNNLS.2025.3586694.
- 108. Bai F, Du Y, Huang T, Zhao B. SegVol: universal and interactive volumetric medical image segmentation. In: Advances in Neural Information Processing Systems 37 (NeurIPS 2024). Red Hook (NY): Curran Associates; 2024. p.110746-110783.
- 109. Gao J, Li C, Liu H, et al. LLaVA-Med: training a large language-and-vision assistant for biomedicine in one day. In: Advances in Neural Information Processing Systems 36 (NeurIPS 2023). Red Hook (NY): Curran Associates; 2023. p.28541-28564.
- 110. Tu T, Azizi S, Driess D. Towards generalist biomedical AI. NEJM AI 2024;1:AIoa2300138.
- 111. Ho J, Jain A, Abbeel P. Denoising diffusion probabilistic models. Adv Neural Inf Process Syst 2020;33:6840-6851.
- 112. Sheller MJ, Edwards B, Reina GA, et al. Federated learning in medicine: facilitating multi-institutional collaborations without sharing patient data. Sci Rep 2020;10:12598.