ABSTRACT
Surgical resection remains the only potentially curative treatment for colorectal liver metastases (CRLM). Locoregional therapies such as transarterial chemoembolization (TACE) and radiofrequency ablation (RFA) are frequently used in patients with limited or borderline resectable liver metastases. However, radiologic response does not always indicate complete tumor eradication. A 77-year-old man with rectosigmoid junction cancer presented with synchronous liver metastases (S6, 7). Combined TACE and RFA were performed for both lesions after multidisciplinary discussion. Follow-up imaging suggested complete radiologic response, and laparoscopic low anterior resection was planned for the primary tumor. Intraoperatively, a suspicious whitish lesion was noted on the liver surface, leading to laparoscopic resection. Histopathological examination confirmed residual viable CRLM with negative margins. This case highlights the limitation of imaging-based response assessment after locoregional therapy and suggests that salvage laparoscopic hepatectomy can provide definitive oncologic management in carefully selected patients.
-
KEYWORDS: Colorectal liver metastasis; Radiofrequency ablation; Transarterial chemoembolization; Salvage hepatectomy; Laparoscopic liver resection
INTRODUCTION
Colorectal cancer is one of the most common malignancies worldwide, and the liver represents the most frequent site of distant metastasis. Colorectal liver metastases (CRLM) develop in up to 50% of patients during the course of the disease [
1]. Surgical resection remains the only potentially curative treatment and is associated with favorable longterm survival outcomes. However, a substantial proportion of patients present with unresectable or borderline resectable liver metastases at the time of diagnosis. In these situations, locoregional therapies such as radiofrequency ablation (RFA), transarterial chemoembolization (TACE), and other image-guided techniques have been increasingly used as alternative or adjunctive treatment strategies [
2]. RFA is widely utilized for small liver metastases due to its minimally invasive nature and acceptable local control rates. TACE may also be applied to induce tumor ischemia or enhance the efficacy of ablative therapy. Despite encouraging radiologic responses, incomplete tumor necrosis and residual viable tumor may occur after locoregional treatment. In some cases, radiologic findings may not accurately reflect the pathological status of the treated lesion [
3]. Herein, we report a case of residual CRLM detected intraoperatively despite favorable radiologic findings following combined TACE and RFA, which was successfully treated with salvage laparoscopic hepatectomy.
CASE
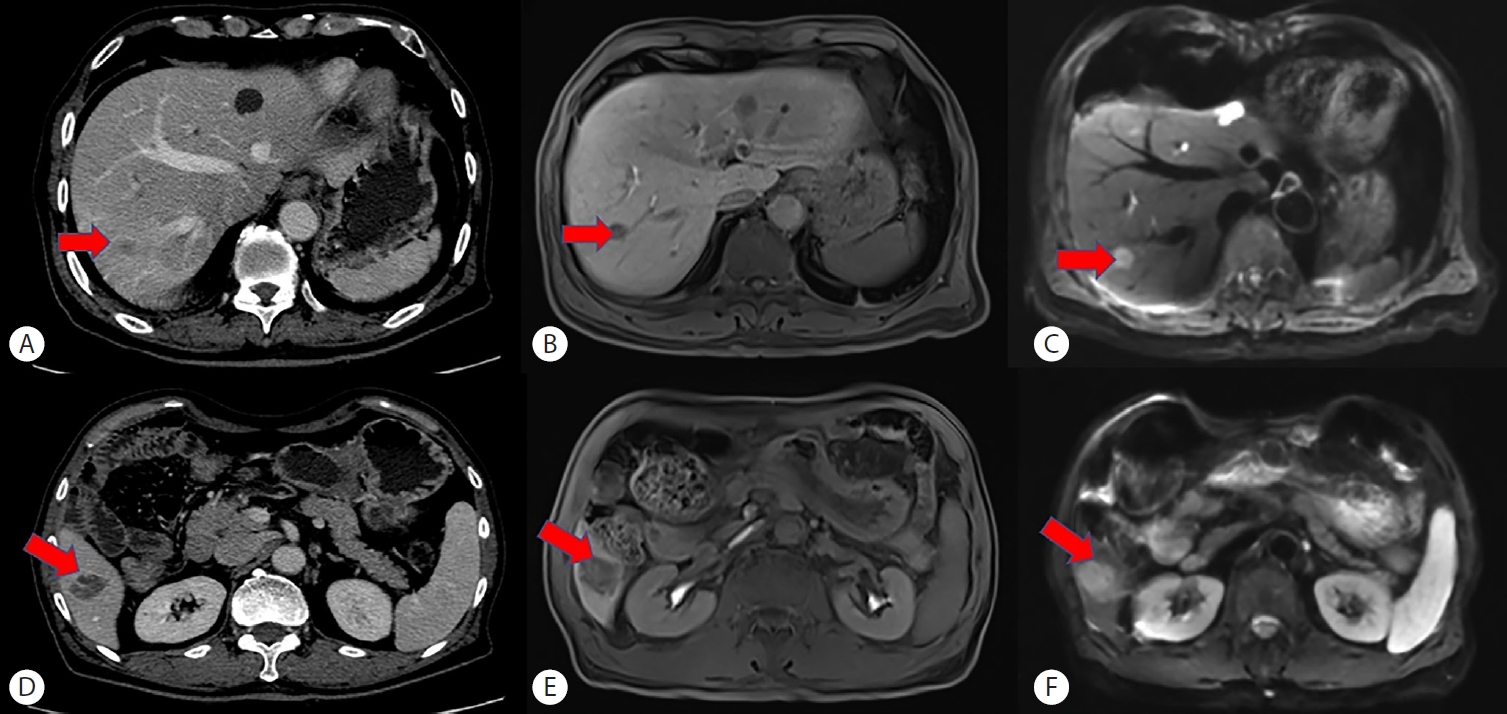
A 77-year-old man was diagnosed with rectosigmoid junction cancer during evaluation for hematochezia. Contrast-enhanced computed tomography (CT) and liver magnetic resonance imaging revealed synchronous liver metastases located at the right hepatic angle measuring 3.3 cm and segment VII measuring 1.2 cm (
Fig. 1). Preoperative laboratory findings revealed elevated tumor marker levels, with carcinoembryonic antigen (CEA) of 15.19 ng/mL and carbohydrate antigen 19-9 (CA 19-9) of 67.50 U/mL, while liver function tests were within normal limits. Although the lesion was considered technically resectable based on the radiologic findings, several limitations were present. The patient had a history of acute myocardial infarction 10 months earlier and had undergone coronary stent insertion, for which triple antithrombotic therapy was being maintained. In addition, prolonged hospital-ization had resulted in marked general weakness. The patient was therefore assessed as having an American Society of Anesthesiologists Physical Status Classification III or higher and an Eastern Cooperative Oncology Group performance status of 3, indicating a high operative risk for major hepatectomy.
Furthermore, both the patient and the caregivers preferred locoregional treatment over hepatic resection if possible. After multidisciplinary discussion with the interventional radiology team, it was decided to proceed with a combination of RFA and TACE, despite the possibility of inferior oncologic efficacy compared with surgical resection. Salvage resection was planned as a potential option in the event of future recurrence.
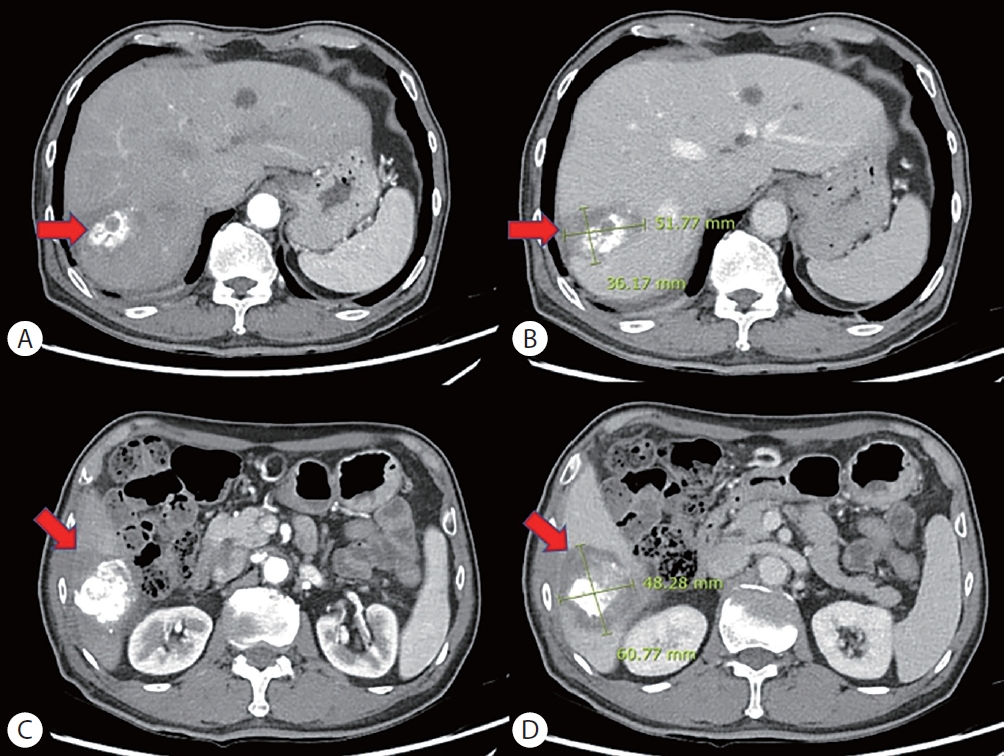
Follow-up imaging demonstrated a favorable treatment response without definite residual enhancing lesions (
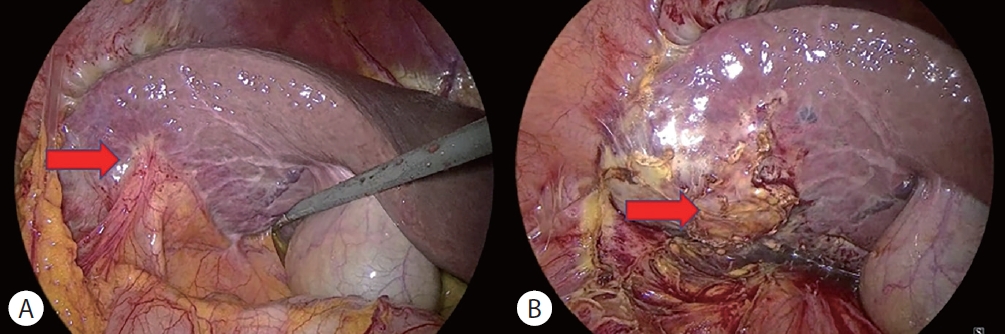
Fig. 2). Based on these findings, laparoscopic low anterior resec-tion was planned for the primary colorectal tumor. During surgery, careful exploration of the liver was performed. A whitish lesion suspicious for residual tumor was identified on the liver surface near segment VI (
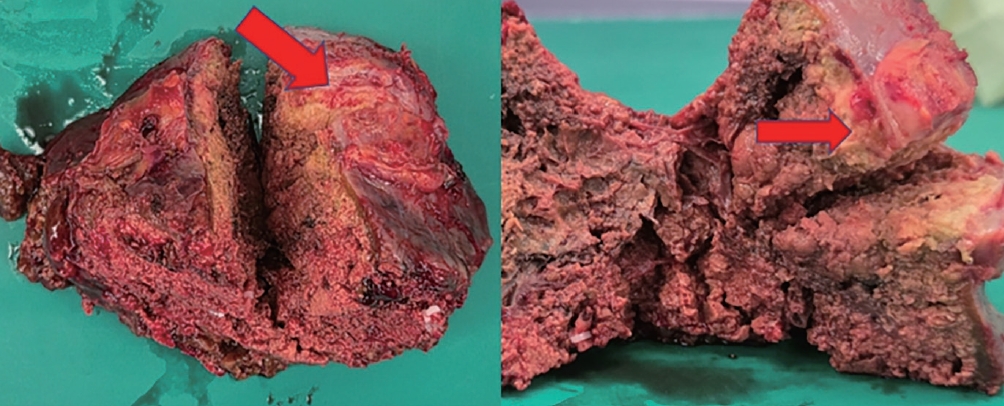
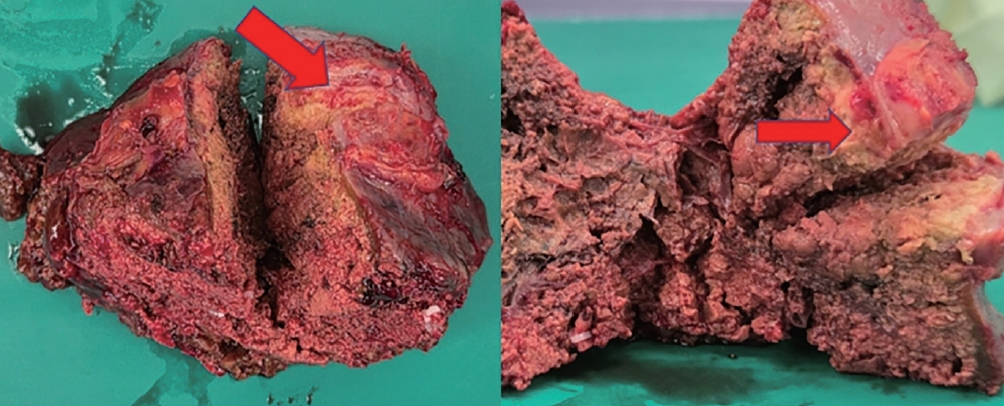
Fig. 3). Considering the possibility of residual metastatic disease, laparoscopic segment VI segmentectomy was additionally performed. By postoperative day 5, laboratory findings had returned to normal ranges. However, intermittent fever developed, and abdominal computed tomography revealed a fluid collection at the liver resection site. Percutaneous catheter drainage was subsequently performed, after which the fever improved. The patient was discharged on postoperative day 12 following resolution of the drainage output and improvement in general condition. Histopathological examination of the resected specimen confirmed residual colorectal liver metastasis with negative surgical margins (
Fig. 4). At the 5-month postoperative follow-up, tumor marker levels had decreased to a CEA level of 1.88 ng/mL and a CA 19-9 level of 26.27 U/mL. Follow-up abdominal CT demonstrated no evidence of recurrence or metastasis.
DISCUSSION
Locoregional therapies have increasingly been incorporated into the management of CRLM, particularly in patients with limited disease burden or those who are not ideal candidates for immediate surgical resection. Among these modalities, RFA has been widely used due to its minimally invasive nature and relatively favorable local control rates for small liver metastases. Previous studies have suggested that RFA may achieve acceptable outcomes when the tumor diameter is less than 3 cm [
4]H. However, tumor size remains one of the most important determinants of local tumor progression after ablation, and the efficacy of RFA alone decreases substantially in lesions larger than 3 cm due to insufficient ablative margins and the heat-sink effect from adjacent vessels. Several studies have demonstrated higher rates of incomplete ablation and local recurrence in larger tumors treated with RFA alone [
5]. To overcome these limitations, TACE has been utilized as an adjunctive treatment for liver metastases. By inducing ischemic necrosis and delivering high concentrations of chemotherapeutic agents to the tumor, TACE may enhance the effect of ablative therapies and reduce tumor vascularity, thereby diminishing the heat-sink effect during thermal ablation. Combination treatment strategies such as TACE followed by RFA have therefore been proposed to improve tumor control in selected cases, particularly for tumors larger than 3 cm. Previous reports evaluating combined embolization and thermal ablation for metastatic liver tumors have suggested that this approach is feasible and may improve local tumor control and survival outcomes compared with ablation alone in selected patients. More recently, studies focusing on CRLM have also suggested that TACE combined with RFA may provide better oncologic outcomes than TACE alone in patients who are poor surgical candidates or have borderline resectable disease [
6-
8].
Nevertheless, despite these theoretical and clinical advantages, complete pathological response cannot always be guaranteed following combination locoregional therapy. Incomplete tumor destruction remains an important limitation of ablative therapy. Several factors including tumor size, tumor location, and the heat-sink effect from adjacent vessels may contribute to residual viable tumor. Previous studies have also reported discrepancies between radiologic response and pathological findings following ablation therapy. In particular, imaging studies may suggest complete response even when microscopic viable tumor persists [
9,
10].
In the present case, follow-up imaging after combined TACE and RFA suggested a favorable response without clear evidence of residual disease. However, intraoperative inspection revealed a suspicious lesion on the liver surface, and histopathological analysis ultimately confirmed residual metastatic tumor. This finding highlights the potential discrepancy between imaging findings and the true pathological status following locoregional therapy. In the present patient, surgical resection had initially been considered technically feasible. However, the patient had significant comorbidities, including a recent history of acute myocardial infarction requiring coronary stent insertion and ongoing triple antithrombotic therapy, as well as poor general condition with high operative risk for major hepatectomy. Therefore, combined TACE and RFA was selected as an alternative treatment strategy. This case demonstrates that although combination locoregional therapy may serve as a valuable therapeutic option in highrisk patients with larger CRLM, careful surveillance remains mandatory because radiologic complete response may not accurately reflect complete tumor eradication.
Another noteworthy aspect of this case is the feasibility of salvage laparoscopic hepatectomy. With advances in minimally invasive liver surgery, laparoscopic hepatectomy has become an established treatment option for selected patients with CRLM. In experienced centers, laparoscopic liver resection has demonstrated comparable oncologic outcomes to open surgery while providing the benefits of minimally invasive surgery, including reduced postoperative pain and shorter hospital stay [
11-
13].
This case underscores several important clinical implications. First, radiologic response after locoregional therapy does not necessarily indicate complete tumor eradication. Second, careful intraoperative assessment remains essential when previously treated lesions are present. Finally, salvage surgical resection should be considered when residual disease is suspected, as it may offer definitive oncologic treatment [
14].
NOTES
-
ACKNOWLEDGEMENTS
None.
-
FUND
None.
-
ETHICS STATEMENT
Informed consent was obtained from the patient for publi cation of this case report.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Song SH conceived and designed the study, reviewed the literature, and contributed to manuscript drafting and editing; Koh YS contributed to manuscript revision; all authors issued final approval for the version to be submitted and ap proved the publication of the manuscript.
Figure 1.Preoperative CT and MRI demonstrating synchronous colorectal liver metastases. Portal venous phase CT (A, D), hepatobiliary phase MRI (B, E), and diffusion-weighted imaging (C, F) identify two lesions: a 3.3-cm mass at the right hepatic angle (A–C) and a 1.2-cm lesion in segment VII (D–F) (arrows). CT, computed tomography; MRI, magnetic resonance imaging.
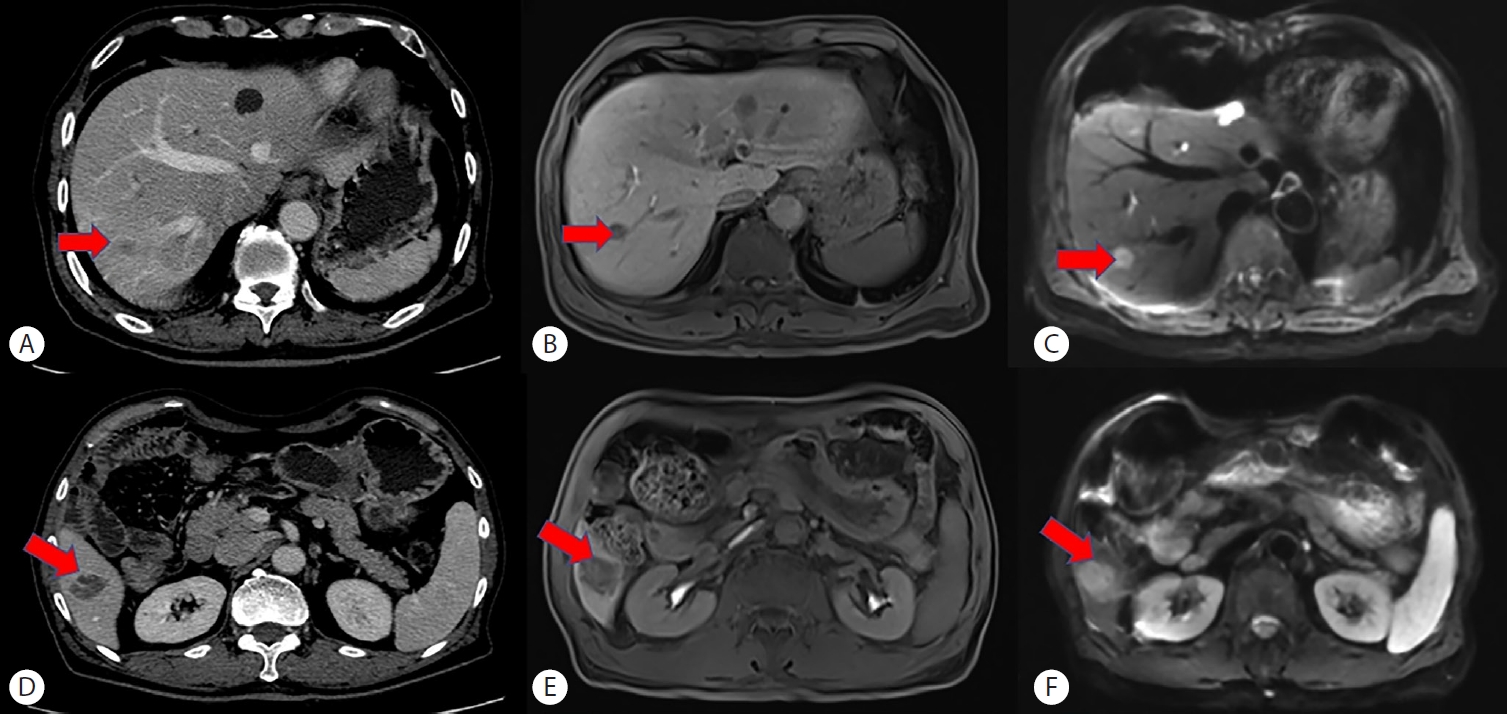
Figure 2.Follow-up dynamic CT after TACE and RFA. Arterial phase (A, C) and portal venous phase (B, D) images demonstrate treated lesions without definite residual arterial enhancement, indicating an apparent radiologic response (arrows). CT, computed tomography; RFA, radiofrequency ablation; TACE, transarterial chemoembolization.
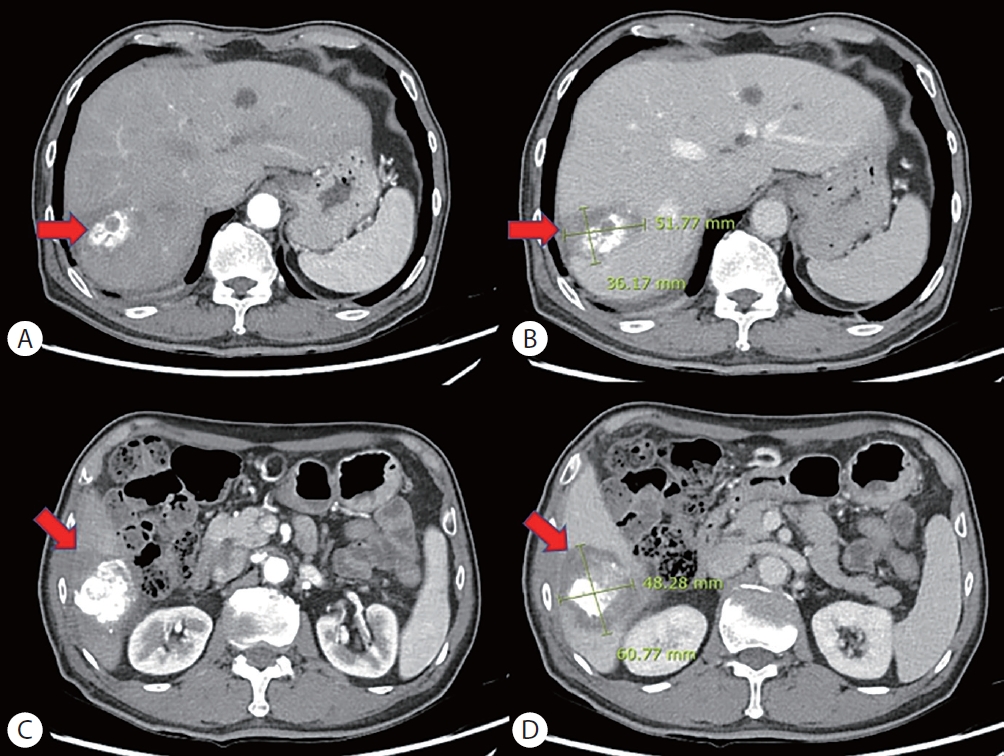
Figure 3.Intraoperative laparoscopic findings after TACE and RFA. A whitish lesion on the liver surface near segment VI (A) was identified, raising suspicion for residual tumor. Frozen-section biopsy confirmed adenocarcinoma (B), and segment VI segmentectomy was subsequently performed (arrows). RFA, radiofrequency ablation; TACE, transarterial chemoembolization.
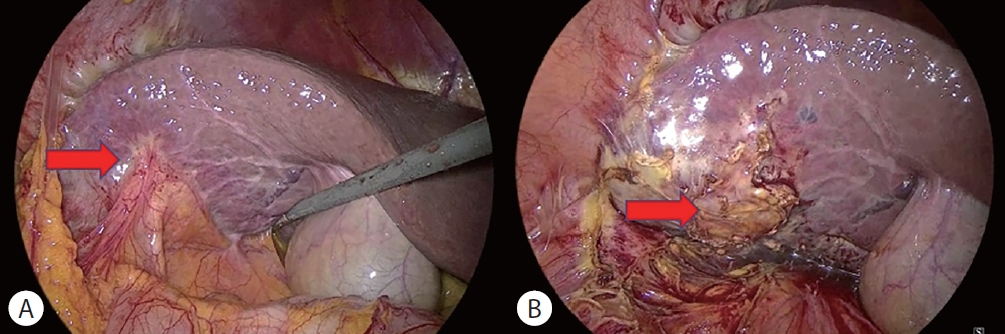
Figure 4.Gross appearance of the resected liver specimen after segment VI segmentectomy. A whitish area on the cut surface (arrows) corresponds to the treated lesion, in which histopathology confirmed residual colorectal liver metastasis. An adequate resection margin was achieved.
REFERENCES
- 1. Qian Y, Li Y, Fu Y. A commentary on “Prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer liver metastasis: a meta-analysis of results from multivariate analysis”. Int J Surg 2023;109:2823-2824.
- 2. Seager MJ, Jakobs TF, Sharma RA, Bandula S. Combination of ablation and embolization for intermediate-sized liver metastases from colorectal cancer: what can we learn from treating primary liver cancer? Diagn Interv Radiol 2021;27:677-683.
- 3. Shady W, Petre EN, Gonen M, et al. Percutaneous radiofrequency ablation of colorectal cancer liver metastases: factors affecting outcomes--a 10-year experience at a single center. Radiology 2016;278:601-611.
- 4. Sun Y, Jiang S, Wu R, Zhou B. Radiofrequency ablation for colorectal liver metastases: an evolving alternative or complement to resection? Hepatobiliary Surg Nutr 2025;14:1034-1037.
- 5. Vulasala SSR, Sutphin PD, Kethu S, Onteddu NK, Kalva SP. Interventional radiological therapies in colorectal hepatic metastases. Front Oncol 2023;13:963966.
- 6. Faiella E, Calabrese A, Santucci D, et al. Combined trans-arterial embolization and ablation for the treatment of large (>3 cm) liver metastases: review of the literature. J Clin Med 2022;11:5576.
- 7. Vogl TJ, Freichel J, Gruber-Rouh T, et al. Interventional treatments of colorectal liver metastases using thermal ablation and transarterial chemoembolization: a single-center experience over 26 years. Cancers (Basel) 2024;16:1756.
- 8. Kobe A, Tselikas L, Deschamps F, et al. Single-session transarterial chemoembolization combined with percutaneous thermal ablation in liver metastases 3 cm or larger. Diagn Interv Imaging 2022;103:516-523.
- 9. Franke J, Rosiak G, Konecki D, Milczarek K, Cieszanowski A. Technical aspects, methodological challenges, and factors predicting outcomes of percutaneous ablation for colorectal liver metastases. Pol J Radiol 2025;90:e279-e285.
- 10. Xenos D, Sotirchos VS, Dimopoulos PM, Sofocleous CT. Interventional oncology for colorectal liver metastases: From local cure to salvage therapy. Biomedicines 2025;13:2182.
- 11. Todeschini L, Caimano M, Mattia A, et al. Radiofrequency ablation versus surgical resection in colorectal liver metastasis: insight from an umbrella review. Front Oncol 2025;15:1494996.
- 12. Folkerts AD, Janczewski LM, Merkow RP. Liver-directed therapies for colorectal liver metastases. Cancer 2025;131:e70097.
- 13. Torielli P, McGale J, Liao MJ, et al. Hepatic metastases management: A comparative review of surgical resection, thermal ablation, and stereotactic body radiation therapy. Eur J Cancer 2025;228:115691.
- 14. Alotaibi A, Alshamrani G, Alzobaidi H, et al. A comparison of fiveyear survival rates between thermal ablation and hepatic resection for colorectal cancer metastasis to the liver: a systematic review and meta-analysis. World J Oncol 2025;17:95-105.
Citations
Citations to this article as recorded by