ABSTRACT
Newly detected hepatic lesions during surveillance in patients with a history of breast cancer are often suspected to represent metastatic disease; however, benign infectious conditions, including parasitic infections, may rarely mimic malignancy on imaging. A 48-year-old woman with a history of breast cancer who had undergone curative surgery was found to have a new hepatic lesion on routine surveillance imaging. Magnetic resonance imaging demonstrated a 1.1-cm irregular mass at the hepatic dome with peripheral enhancement, raising suspicion for metastasis. Laparoscopic wedge resection of the segment VIII lesion was performed for definitive diagnosis. Histopathologic examination revealed a necrotizing granuloma containing degenerated parasitic larvae with eosinophilic inflammatory infiltrates and no evidence of malignancy. The findings were most consistent with Capillaria hepatica infection, highlighting that parasitic necrotizing granuloma may be considered as a rare differential diagnosis in patients with prior malignancy.
-
KEYWORDS: Breast neoplasms; Liver neoplasms; Granuloma; Parasitic diseases; Capillaria hepatica
INTRODUCTION
In patients with a history of breast cancer, newly detected hepatic lesions during surveillance imaging are often presumed to represent metastasis, even when the lesion is small [
1]. However, several benign conditions may mimic metastatic disease, including inflammatory or infectious etiologies [
2,
3]. Among them, parasitic infection involving the liver is uncommon but can present as a solitary mass-like lesion with nonspecific radiologic features.
Necrotizing granuloma is a representative histopathologic pattern of hepatic parasitic infection, and its diagnosis may be challenging when serologic tests are negative and peripheral eosinophilia is absent. In such situations, tissue confirmation is essential to avoid misdiagnosis and inappropriate oncologic management [
4-
6].
Herein, we report a case of a small solitary hepatic lesion detected during breast cancer surveillance that mimicked metastasis on magnetic resonance imaging (MRI) but was ultimately diagnosed as a parasitic necrotizing granuloma after laparoscopic wedge resection.
CASE
A 48-year-old woman with a history of breast cancer status post curative surgical treatment was referred for evaluation of a newly detected hepatic lesion identified on surveillance imaging. The patient was asymptomatic and denied abdominal pain, fever, or weight loss.
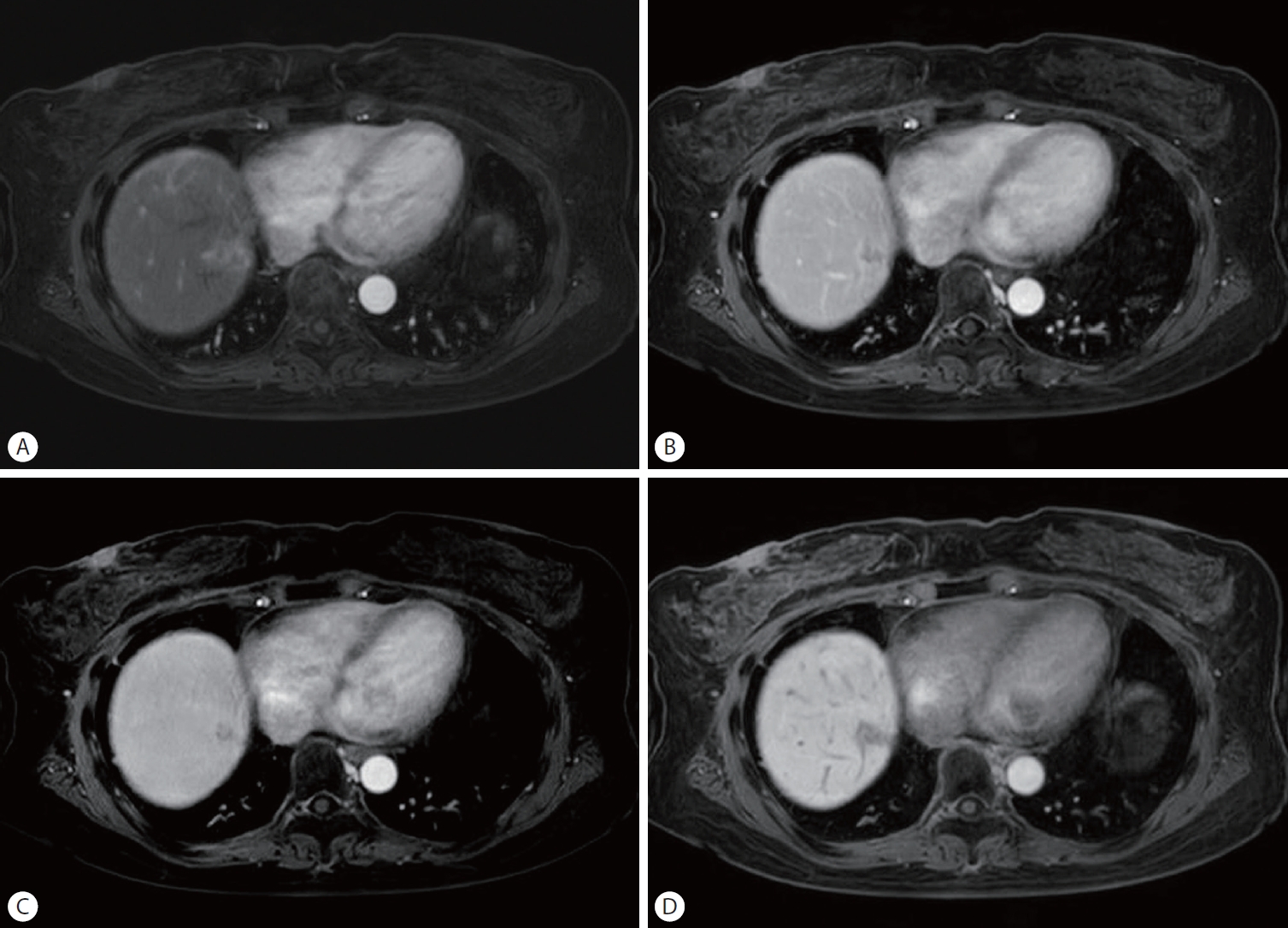
Abdominal imaging revealed a newly developed hepatic lesion. MRI demonstrated an approximately 1.1-cm irregular mass at the hepatic dome (
Fig. 1). The lesion showed peripheral enhancement in the arterial phase (
Fig. 1A). No definite washout was identified in the portal venous and delayed phases (
Fig. 1B,
1C). In the hepatobiliary phase, the lesion appeared relatively hypointense compared with the surrounding liver parenchyma (
Fig. 1D). These imaging features were considered indeterminate but raised suspicion for metastatic disease in the context of the patient’s oncologic history. The patient reported frequent consumption of raw seafood within the previous 6 months. Preoperative laboratory tests did not demonstrate any significant abnormalities. Liver function tests were within normal limits (aspartate aminotransferase 28 U/L, alanine aminotransferase 18 U/L, total bilirubin 0.70 mg/dL), and coagulation parameters were normal (international normalized ratio 0.98), without peripheral eosinophilia (eosinophils 2.3%).
Given the patient’s oncologic history and imaging findings suspicious for metastasis, laparoscopic wedge resection of the hepatic segment VIII lesion was performed to obtain a definitive diagnosis. Intraoperatively, the lesion was located at the hepatic dome superior to the right hepatic vein, and an additional trocar was required for safe exposure and resection. The postoperative course was uneventful, and the patient was discharged on postoperative day 5.
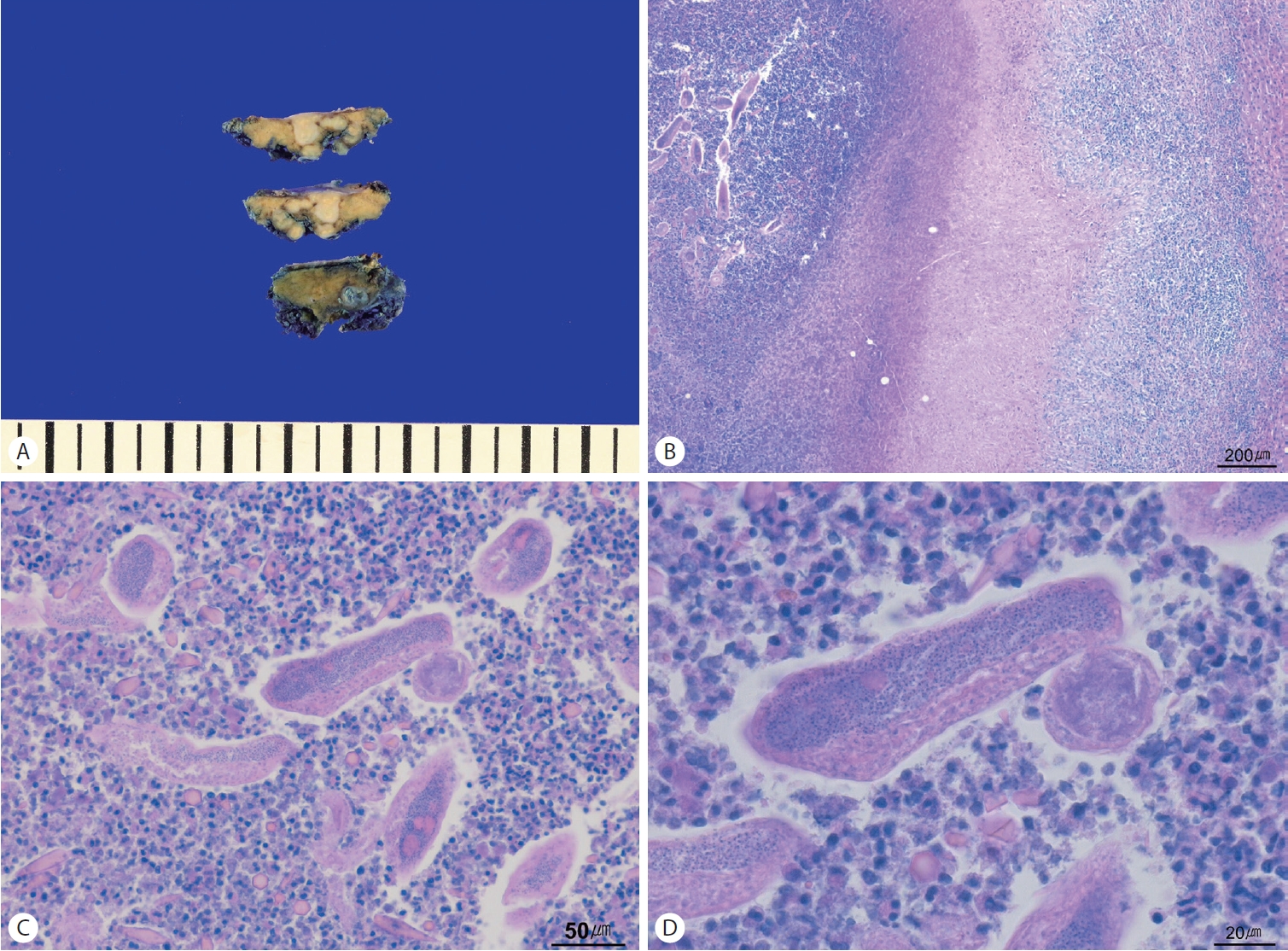
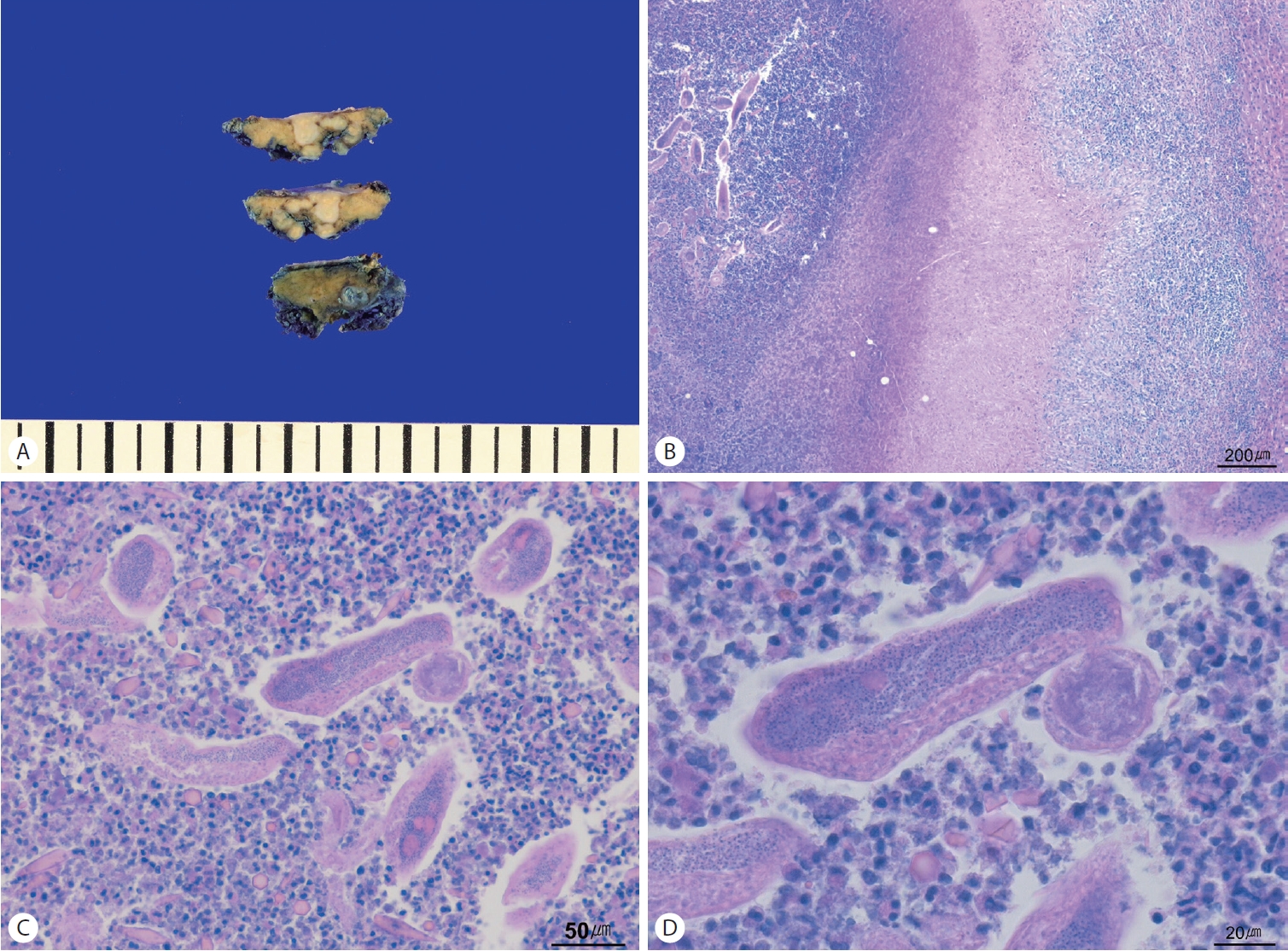
Histopathologic evaluation demonstrated a localized yellowish necrotic lesion on gross examination (
Fig. 2A). Low-power microscopy revealed a well-demarcated necrotizing granuloma with central coagulative necrosis (
Fig. 2B). At higher magnification, degenerated parasitic larvae/worm fragments were identified within the necrotic core, surrounded by granulomatous inflammation with prominent eosinophilic infiltration (
Fig. 2C,
2D). No evidence of malignancy was identified.
Additional microbiologic evaluation, including polymerase chain reaction for Mycobacterium tuberculosis and non-tuberculous mycobacteria, was negative. Serologic tests for cysticercus, paragonimus, clonorchis, toxoplasma, and sparganum were all negative. Based on expert review, the findings were considered most consistent with Capillaria hepatica infection.
The patient did not receive antiparasitic therapy and remained well without recurrence or new lesions during approximately 1 year of follow-up.
DISCUSSION
This case illustrates a rare but clinically important diagnostic pitfall: a small solitary hepatic lesion detected during breast cancer surveillance that mimicked metastatic disease on imaging but was ultimately proven to be a parasitic necrotizing granuloma. In oncology patients, newly identified hepatic lesions often prompt strong suspicion for metastasis, even when the lesion is small, because accurate staging has critical implications for prognosis and treatment [
1]. However, benign conditions may present with overlapping radiologic features, and infectious etiologies should be considered in the differential diagnosis [
2,
3].
In the present case, MRI demonstrated an approximately 1.1-cm irregular mass with peripheral enhancement at the hepatic dome, a finding that can be compatible with metastatic disease. The lesion was incidentally detected and the patient was asymptomatic with preserved liver function, normal coagulation profiles, and no peripheral eosinophilia. Despite the absence of systemic inflammatory signs, the patient’s dietary history supported the possibility of parasitic exposure. Nevertheless, noninvasive investigations alone were insufficient to confidently exclude malignancy in this clinical setting. Definitive diagnosis was achieved through laparoscopic wedge resection and histopathologic evaluation. In this case, percutaneous core needle biopsy (PCNB) was not performed prior to surgery. This decision was based on several considerations. First, the small size of the lesion and the presence of central necrosis raised concern for limited diagnostic yield and potential sampling error with PCNB. Second, the lesion was located at the hepatic dome adjacent to the inferior vena cava, making percutaneous access technically challenging and potentially unsafe. In addition, given the patient’s history of malignancy, obtaining a definitive diagnosis was considered essential for accurate staging and treatment planning. Therefore, surgical resection was selected as both a diagnostic and potentially therapeutic approach. The resected specimen showed a necrotizing granuloma containing degenerated parasitic larvae/worm fragments with surrounding granulomatous inflammation and eosinophilic infiltration. Importantly, no evidence of malignancy was identified. These findings highlight that histopathology provides the most direct and reliable evidence for parasitic infection in cases of focal hepatic lesions, particularly when imaging findings are nonspecific and malignancy is a major concern.
The negative serologic results for multiple parasites warrant careful interpretation. Although serologic testing may be useful as an ancillary diagnostic tool, negative serology does not exclude a parasitic etiology. Reported sensitivities of serologic assays vary widely depending on the parasite species and stage of infection, and may be limited due to cross-reactivity and variability in host immune responses. Therefore, serologic results should be interpreted in conjunction with clinical, laboratory, and radiologic findings [
7]. Serologic tests may have limited sensitivity depending on the parasite species, timing of infection, parasite burden, host immune response, and the availability of organism-specific assays. Moreover, routine screening panels may not cover all possible causative organisms. In this case, expert review suggested
Capillaria hepatica infection as the most likely etiology, which may not be reliably detected by commonly performed serologic tests [
3,
5,
6,
8].
Another noteworthy aspect of this case is that antiparasitic therapy was not administered. This management approach was considered reasonable because the lesion was completely excised, the patient remained asymptomatic with unremarkable laboratory findings, and there was no evidence of recurrence or new hepatic lesions during approximately 1 year of follow-up.
From a surgical perspective, laparoscopic wedge resection was performed safely despite the challenging location at the hepatic dome near the right hepatic vein, requiring an additional trocar for appropriate exposure. This case supports the role of minimally invasive surgery in the management of small indeterminate hepatic lesions when tissue diagnosis is required, potentially preventing unnecessary systemic therapy or incorrect oncologic staging in cancer survivors [
9-
11].
In conclusion, parasitic necrotizing granuloma may be considered as a rare differential diagnosis for small hepatic lesions in patients with a history of malignancy. Even in the absence of peripheral eosinophilia and despite negative serologic tests, parasitic infection cannot be excluded. Surgical resection can provide a definitive diagnosis and may be curative in selected patients with solitary lesions.
NOTES
-
ACKNOWLEDGEMENTS
None.
-
FUND
None.
-
ETHICS STATEMENT
Consent for publication is not required, as this submission does not include any images or information that could identify any individual.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: Chan Woo Cho. Data curation: Do Hyeon Lee, Chan Woo Cho. Writing – original draft: Do Hyeon Lee.
Figure 1.Magnetic resonance imaging findings of the hepatic lesion. (A) Arterial phase, (B) portal venous phase, (C) delayed phase, and (D) hepatobiliary phase.
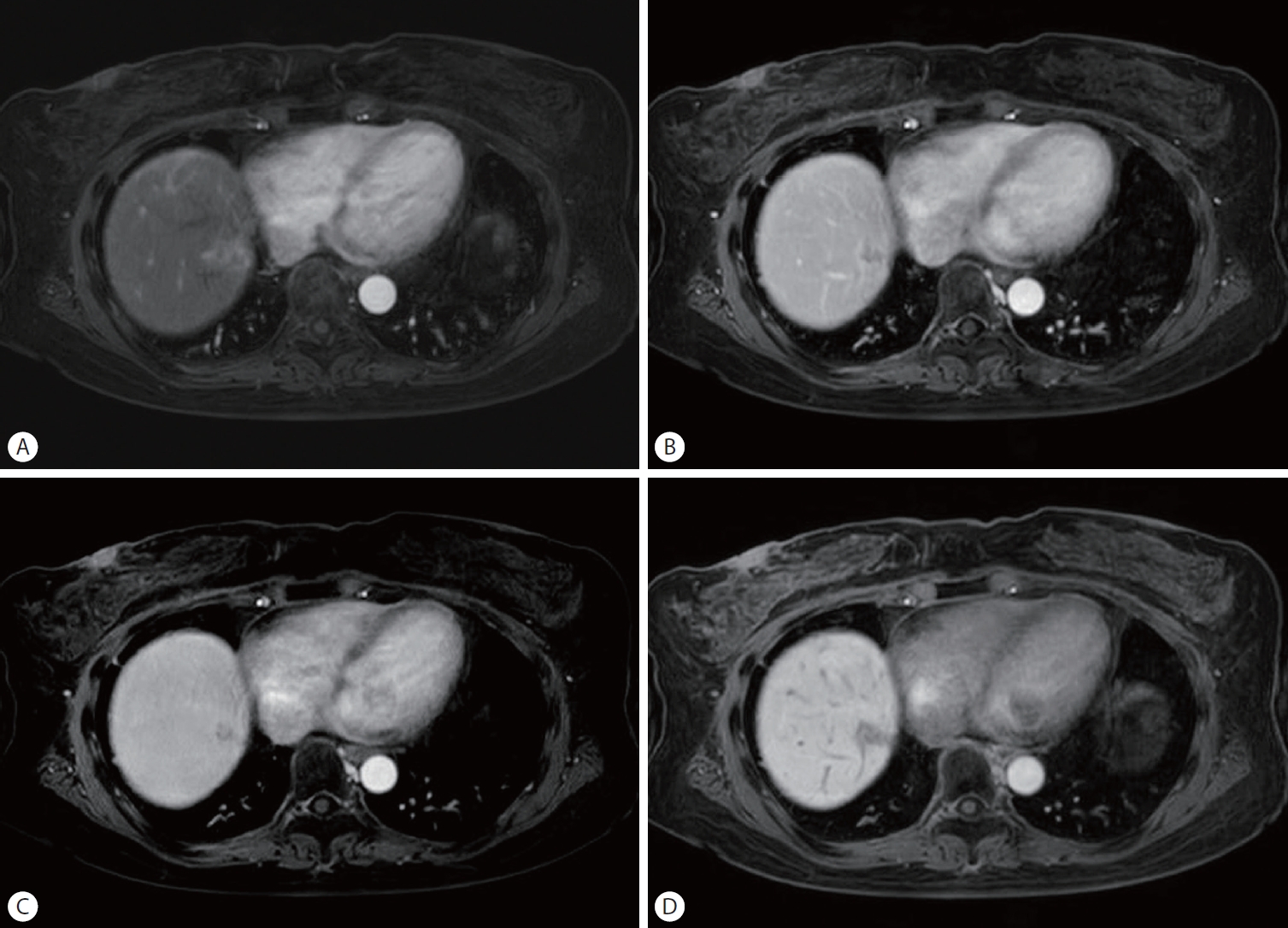
Figure 2.Gross specimen and histopathologic findings of parasitic necrotizing granuloma. (A) Gross photograph of the resected hepatic specimen, (B) low-power view, (C) intermediate-power view, and (D) high-power view (hematoxylin and eosin stain; B, ×40; C, ×200; D, ×400).
REFERENCES
- 1. Granata V, Fusco R, Simonetti I, et al. MRI management of focal liver lesions: what a beginner cannot fail to know. Front Oncol 2025;15:1630424.
- 2. You SH, Park BJ, Kim YH. Hepatic lesions that mimic metastasis on radiological imaging. Korean J Radiol 2017;18:413-426.
- 3. Danet IM, Semelka RC, Leonardou P, et al. Spectrum of MRI appearances of untreated metastases of the liver. AJR Am J Roentgenol 2003;181:809-817.
- 4. Lagana SM, Moreira RK, Lefkowitch JH. Hepatic granulomas: pathogenesis and differential diagnosis. Clin Liver Dis 2010;14:605-617.
- 5. Coash M, Forouhar F, Wu CH, Wu GY. Granulomatous liver diseases: a review. J Formos Med Assoc 2012;111:3-13.
- 6. Lamps LW. Hepatic granulomas: a review with emphasis on infectious causes. Arch Pathol Lab Med 2015;139:867-875.
- 7. Choi M. Serological diagnosis of tissue-invading parasites in Korea. Ann Clin Microbiol 2024;27:81-91.
- 8. Kazemi Aghdam M, Karimi A, Amanati A, et al. Capillaria hepatica: A case report and review of the literature. Arch Pediatr Infect Dis 2015;3:e19398.
- 9. Uchida Y, Yokoyama K, Higashi T, et al. Eosinophilic granuloma of the liver mimicking metastatic liver tumor: a case report. Intern Med 2022;61:1511-1517.
- 10. Choudhury S, Agrawal A, Mohite A, et al. Granulomatous hepatitis masquerading as metastases on FDG PET/CT. Eur J Nucl Med Mol Imaging 2020;47:1013-1014.
- 11. Bekki T, Yamamoto Y, Saeki Y, Arihiro K, Tanabe K, Ohdan H. Iatrogenic hepatic granuloma suspected as liver metastatic lesion: a case report. Clin Case Rep 2020;8:2353-2357.
Citations
Citations to this article as recorded by